Back to Basics: Fever, Cough, SOB
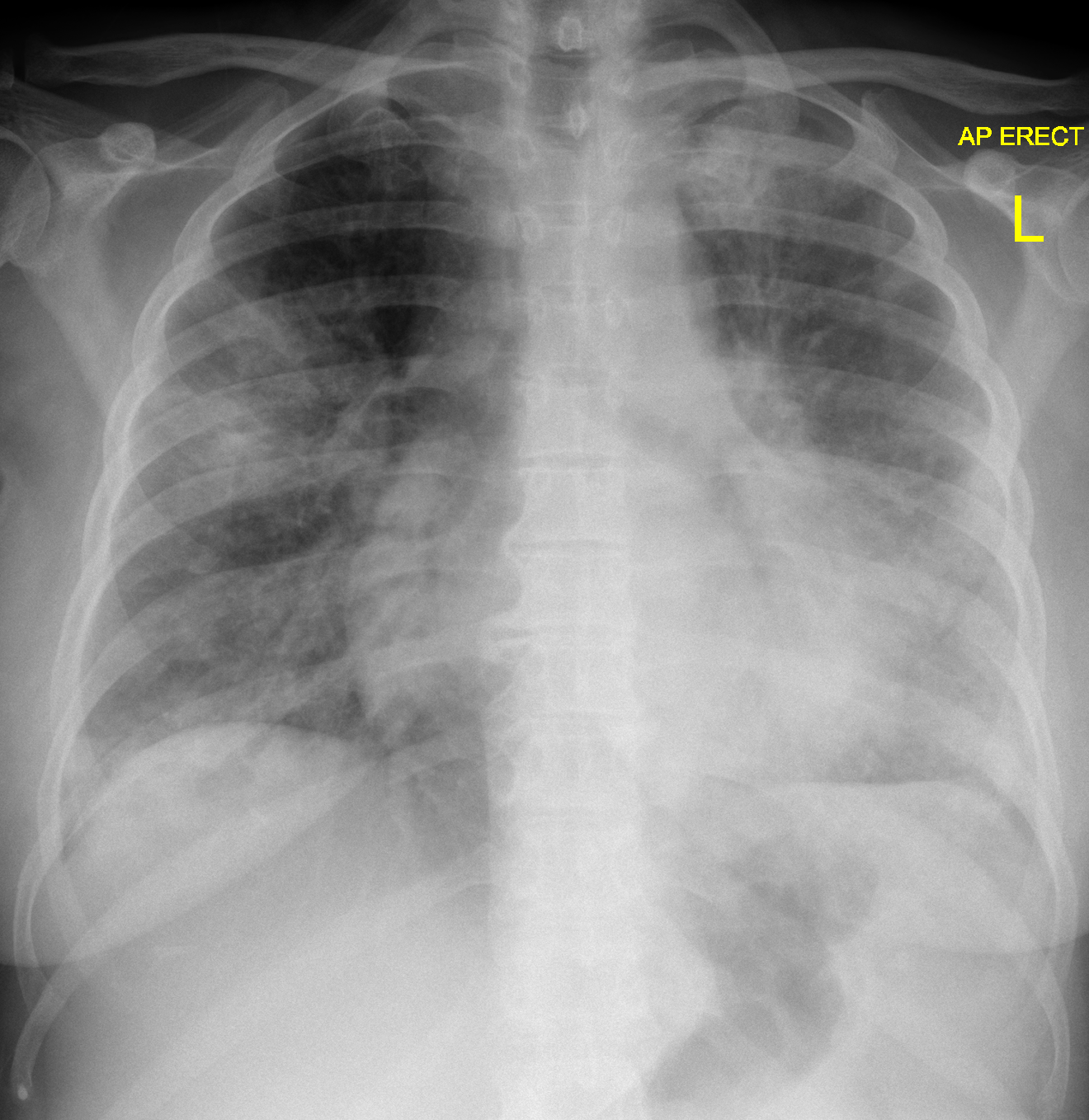
A patient comes into the ED with a high fever, shortness of breath, mild headache, diarrhea, and general malaise. It’s 2021… so naturally, the ‘COVID alarms’ start sounding in our heads. CXR on arrival is shown below.
You stabilize the patient and a few hours later, the COVID PCR comes back negative. Rapid influenza A & B tests are also negative.
Could it still be COVID? Absolutely. Could it be something else? Definitely.
Remember that ‘SS Cysteine’ drawing from Sketchy Micro? I’ll give you a hint, it involves sailors having similar symptoms...
That’s right - Legionella!
Remember, Legionella can cause 2 (technically 3) syndromes…
1) Legionnaires' disease - a pneumonia caused by Legionella species
2) Pontiac fever - an acute, self-limited febrile illness typically acquired during outbreaks (no respiratory symptoms)
3) Extrapulmonary legionellosis (very rare - cellulitis, endocarditis, peritonitis, etc)
‘Legionnaires’ Disease’ Basics
- Clinical Presentation - fever (as high as 105F), fatigue, cough, shortness of breath, +/- GI symptoms (nausea, vomiting, diarrhea), +/- neurologic symptoms (confusion, AMS)
- The patient may also be bradycardic or have a normal pulse rate, despite having a high fever & hypoxia!
- Labs - hyponatremia, elevated transaminases
- CXR - patchy unilobar infiltrates, which can progress to consolidations
- Transmission - via inhalation aerosols from contaminated water or soil
- Patients can get community acquired or nosocomial (hospital acquired) infections.
- Incubation Period - typically 4-6 days
- Risk Factors - smoking, age (most patients are >50 y/o), immunosuppression, chronic cardiopulmonary or renal disease, exposure to contaminated manmade water reservoir(s) (ie showers, hot tubs, pools, etc)
- Diagnosis - rapid urine antigen test- typically results in 1 hour or less, has a 99% specificity, andshould remain positive for weeks after symptom onset!
- Treatment - azithromycin or levofloxacin
- Complications - rhabdomyolysis & renal failure (watch for rising creatinine, hematuria, muscle aches/pain)
TLDR - Though less common than COVID, don’t forget about Legionella as a possible cause of your patient’s CAP. Per UpToDate, all patients with moderate to severe CAPor patients with CAP who require hospitalization should be tested!
References:
Murdoch D et al. Clinical manifestations and diagnosis of Legionella infection. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. (Accessed on February 19, 2021.)
Murdoch D et al. Treatment and prevention of Legionella infection. In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA. (Accessed on February 19, 2021.)
Edelstein PH and Roy CR. Legionnaires' Disease and Pontiac Fever. In: Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases, 8, Bennet JE, Dolin R and Blaser MJ (Eds), Elsevier, Pennsylvania 2015.
Marston BJ, Lipman HB, Breiman RF. Surveillance for Legionnaires' disease. Risk factors for morbidity and mortality. Arch Intern Med 1994; 154:2417.
Den Boer JW, Nijhof J, Friesema I. Risk factors for sporadic community-acquired Legionnaires' disease. A 3-year national case-control study. Public Health 2006; 120:566.
Sutarjono B, Alexis J, Sachidanandam JC. Legionella pneumonia complicated by rhabdomyolysis. BMJ Case Reports CP 2019;12:e229243.
Legionella pneumonia. In: Radiopaedia, online. Accessed on February 19, 2021.