Back to Basics: Insulin Quick & Dirty in the ED (Part 1)
Insulin Part 1 - Quick and dirty in the ED
By: Rachel Rafeq, PharmD & Karen O'Brien, DO
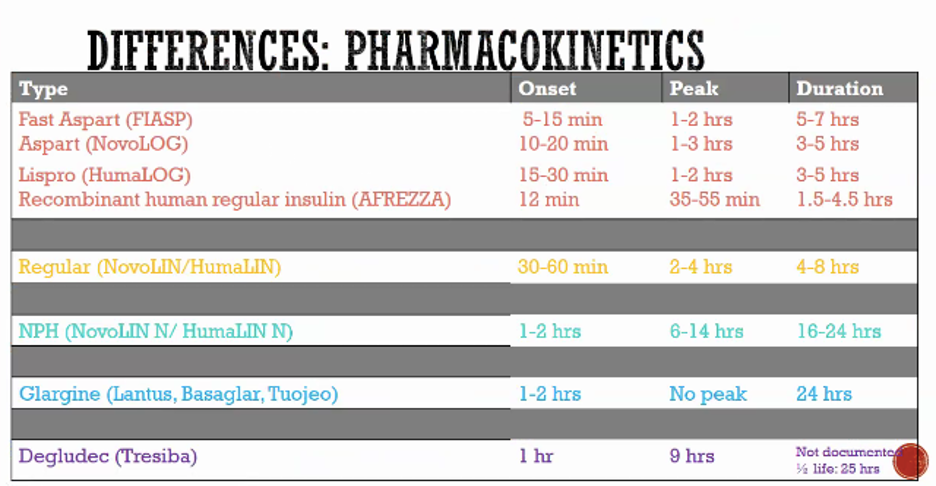
- Short acting (-LIN) > actually just regular insulin that mimics our body’s baseLINe insulin
o Humulin R (R = regular)
o Novolin R
- Rapid acting = Humalog (lispro), novolog (aspart), glulisine
o Quick on quick off mealtime insulin
- Ultra rapid acting = FIASP (aspart), Afrezza
- Humulin N (NPH) = iNtermediate
o Acts longer
- Long acting = glargine or detemir
o 24 hours peakless
- Ultra-long = 25 hours half-life
- Mixed products such as insulin NPH suspension with regular (Humulin 70/30 or Novolin 70/30)
- Most insulins are injected but there is also an inhaled recombinant human regular insulin called Afrezza
PEARL:
- Standard concentration of insulin = 100 units per 1 mL
- Enter… insulin syringes - to avoid overdosing!
- But don’t use insulin syringes (markings are in units not mL) to dose concentrated insulin
- *Insulin syringes are designed to deliver 100 units for every 1 mL. In a patient receiving U-500 concentrated insulin the dose by nature is 5x more concentrated. This means that if an insulin syringe is utilized, it will deliver an overdose of an already concentrated medication.
- Ex. Patient takes U-500 regular insulin 170 units daily
- With an insulin syringes 170 units = 1.7 mL > 1.7 mL of U-500 is 850 units! Therefore use of tuberculin syringe to draw up the dose which has markings by volume!
References
Hirsch IB, Juneja R, Beals JM, Antalis CJ, Wright EE. The Evolution of Insulin and How it Informs Therapy and Treatment Choices. Endocr Rev. 2020;41(5):733-755. doi:10.1210/endrev/bnaa015
Lexicomp Online, Pediatric and Neonatal Lexi-Drugs Online, Hudson, Ohio: UpToDate, Inc.; 2013; April 15, 2013
LaRue HA, Peksa GD, Shah SC. A Comparison of Insulin Doses for the Treatment of Hyperkalemia in Patients with Renal Insufficiency. Pharmacotherapy. 2017;37(12):1516-1522. doi:10.1002/phar.2038
Moussavi K, Nguyen LT, Hua H, Fitter S. Comparison of IV Insulin Dosing Strategies for Hyperkalemia in the Emergency Department. Crit Care Explor. 2020;2(4):e0092. Published 2020 Apr 29. doi:10.1097/CCE.0000000000000092
Laskey D, Vadlapatla R, Hart K. Stability of high-dose insulin in normal saline bags for treatment of calcium channel blocker and beta blocker overdose. Clin Toxicol (Phila). 2016;54(9):829-832. doi:10.1080/15563650.2016.1209766
Moussavi K, Fitter S, Gabrielson SW, Koyfman A, Long B. Management of Hyperkalemia With Insulin and Glucose: Pearls for the Emergency Clinician. J Emerg Med. 2019;57(1):36-42. doi:10.1016/j.jemermed.2019.03.043
Driver BE, Klein LR, Cole JB, Prekker ME, Fagerstrom ET, Miner JR. Comparison of two glycemic discharge goals in ED patients with hyperglycemia, a randomized trial. Am J Emerg Med. 2019;37(7):1295-1300. doi:10.1016/j.ajem.2018.09.053
Driver BE, Olives TD, Bischof JE, Salmen MR, Miner JR. Discharge Glucose Is Not Associated With Short-Term Adverse Outcomes in Emergency Department Patients With Moderate to Severe Hyperglycemia. Ann Emerg Med. 2016;68(6):697-705.e3. doi:10.1016/j.annemergmed.2016.04.057
Munoz C, Villanueva G, Fogg L, et al. Impact of a subcutaneous insulin protocol in the emergency department: Rush Emergency Department Hyperglycemia Intervention (REDHI). J Emerg Med. 2011;40(5):493-498. doi:10.1016/j.jemermed.2008.03.017