Back to Basics: Succinylcholine and Hyperkalemia
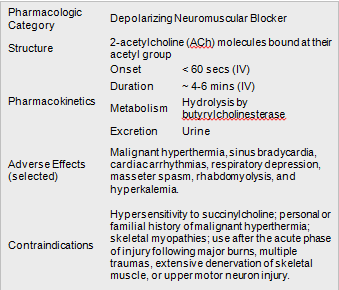
The Med: Succinycholine
The Site: Nicotinic Receptors
•The mature (junctional) nAChR is a ligand-gated channel located on the motor end plate of the neuromuscular junction (NMJ)
•Primary ligand of nAChR is ACh; activation requires the binding of two ACh molecules
•Influx of Na+ and efflux of K+ causes depolarization of the motor end plate potential and subsequent generation of a muscle action potential
In prolonged states of muscle disuse, severe trauma, or denervation, the upregulation of cellular machinery increases the proliferation of immature (extrajunctional) nAChR. The immature nAChR is similar to the mature nAChR, except:
•Located anywhere along the muscle tissue, including the NMJ
•Up to a 10-fold increase in mean channel open time relative to the mature isoform
•Resistant to non-depolarizing neuromuscular blockade and increased sensitivity to succinylcholine
The Adverse Effect: Hyperkalemia
The expected increase of 0.5 mEq/dL is associated with the normal efflux of K+ of the activated nAChR channel. The slight increase is generally benign, occurs within 5 minutes of administration, and in one randomized study, resolved to 90% of initial level within 12 minutes after discontinuance of succinylcholine. Examples of conditions that increase the proliferation of extrajunctional nAChRs and thus, lead to an exaggerated hyperkalemic response in the setting of succinylcholine: stroke, MS, GBS, Hemi/paraplegia, severe burns, spinal cord injury, prolonged immobilization.
Special Considerations: Hypovolemia with Severe Metabolic Acidosis
There is an increased risk of severe hyperkalemia in hypovolemic patients with severe metabolic acidosis. The increased K+ in the metabolic acidosis is linked to the gastrointestinal tract rather than skeletal muscle.
Management of in severe hyperkalemia associated with severe metabolic acidosis.
•Hyperventilation
•1-2 mg IV CaCl
•1 mEq/kg NaHCO3
•10 units regular insulin in 50 mL of 50% glucose
Special Considerations: Severe Burns
•Percent coverage of burn is NOT correlated with the severity of hyperkalemic respons.
•Succinylcholine is safe within 24 hours of a severe burn, as the proliferation of immature nAChR has not yet reached its peak.
•AVOID succinylcholine for 1-2 years following severe burn.
References:
1.Succinylcholine. Lexicomp website. Wolters Kluwer Health, Inc. Riverwoods, IL. http://online.lexi.com. Accessed August 24, 2017.
2.Naquin M, Lien C, Meistelman C. Chapter 34: Pharmacology of Neuromuscular Blocking Drugs. In: Miller's Anesthesia. 8th ed. Philadelphia, PA: Elsevier Inc.; 2015:958-994.
3.Sabo D, Jahr J, Pavlin J, et al. The Increases in Potassium Concentrations are Greater with Succinylcholine than with Rocuronium - Sugammadex in Outpatient Surgery: A Randomized, Multicentre Trial. Canadian Journal of Anesthesia. 2014;61(5):423-32.