The Basics of Ankle Sprains
Ankle sprains are one of the most common traumatic injuries encountered in the Emergency Department. The pathophysiology of an ankle sprain occurs when there is abnormal movement of the talus within the ankle mortise leading to disruption to the surrounding ligaments.
Anatomy:
- Ligaments: Bone-to-bone
- Tendons: Muscle-to-bone
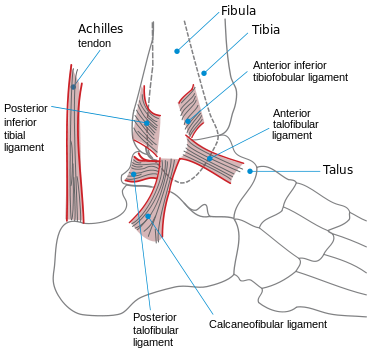
Photo courtesy: https://en.wikipedia.org/wiki/Ankle
Three major ligamentous groups:
- Medial Deltoid:
- Strongest
- Originates at medial malleolus
- Inserts into medial talus, calcaneus, calcaneonavicular ligament, and navicular tuberosity
- Lateral Ligament Complex:
- Components: lateral malleolus, talus and calcaneus
- Lateral malleolus (origin of the ligaments)
- Anterior talofibular ligament [ATFL] (insertion= anterior talus)
- Posterior talofibular ligament (insertion= posterior talus)
- Calcaneofibular Ligament (insertion= calcaneus)
- Anterior talofibular ligament = weakest. Most commonly injured in lateral sprains. Accounts for 85% of all ankle injuries.
- Syndesmosis
- Holds tibia and fibula together
- Carries 16% axial load
- Allows fibula to rotate
- Four distinct ligaments attaching distal tibia to fibula just above the talus:
- Anterior inferior tibiofibular ligament
- Posterior inferior tibiofibular ligament
- Transverse ligament
- Interosseous ligament
Clinical Features of Ankle Sprains
Categories:
- Grade I: No ligamentous tear. Minimal functional loss with pain, swelling or ecchymosis. Can tolerate weight-bearing.
- Grade II: Partial ligamentous tear with some functional loss.
- Grade III: complete ligamentous tear, significant functional loss, pain, swelling, bruising, inability to weight-bear
1. Lateral Ankle Sprains:
Most common ankle sprain and usually a low-grade sprain.
Mechanism: Inversion injury on plantar-flexed foot
Anterior talofibular ligament = most commonly injured ligament.
A positive (laxity) Anterior Draw Test indicates a torn ATFL.
Concomitant calcaneofibular and ATFL ligament injury with ATFL injury can lead to joint instability!
Inversion Stress Test (or Talar Tilt) assesses calcaneofibular ligament instability
Inversion pressure applied to ankle in neutral position. Assess degree of inversion as compared to unaffected side.
Posterior talofibular ligament = strongest of the three lateral ligaments and rarely associated with inversion injuries (most commonly injured with forced dorsiflexion).
Lateral Ankle Sprain Treatment and Disposition:
- If stable joint and weight bearing:
PRICE therapy, analgesics
Supportive bandage (elastic, lace-up ankle brace, aircast boot)
1 week follow up if no improvement in symptoms. - If stable joint and non-weight bearing:
Supportive ankle brace as above with crutches
Follow up with with PCP or orthopedics in 1 week.
- If unstable joint, involve orthopedic consultant prior to discharge.
2. Medial Deltoid Sprains:
Mechanism: eversion injury
Isolated medial deltoid sprains = rare. Usually associated with proximal fibular fracture (Maisonneuve fracture) or syndesmosis injury.
Suspect a Maisonneuve fracture if there is significant medial malleolus tenderness/swelling or proximal fibular shaft/head tenderness.
Negative plain films suggest syndesmosis tears
Medial Deltoid Sprain Treatment and Disposition:
- PRICE
- Early referral to orthopedics (especially because often can present wiht undetected underlying fracture).
- If joint is unstable, apply posterior splint and discuss with orthopedic consultant vs. arrange early follow up with orthopedics.
- Syndesmotic complex sprain have prolonged expected recovery time.
- May need surgical intervention.
3. Syndesmosis Complex Sprains:
Mechanism: Hyperdorsiflexion injuries. The talus moves superiorly and separates the tibia and fibula leading to partial or complete tear of the syndesmosis
Patients with complain of pain just above talus. There is often little ankle edema or ecchymosis.
Crossed leg test: Affected leg is crossed over opposite leg while downward pressure is applied to medial knee of affected side. Pain in syndesmosis area suggest injury.
Squeeze test: Positive test occurs when calf squeeze causes pain in syndesmosis areas.
Additional Clinical Exam Pearls:
- Systematic approach reduces risk of missing injuries.
- Examine joints above and below ankle.
- Check doralis pedis and posterior tibial pulses and assess cap refill.
- Apply Ottawa Ankle Rules to help determine if imaging is needed.
Functional Treatment:
- PRICE Protocol (Protection, Rest, Ice, Compression, Elevation) for up to 72 hrs.
- Functional treatment consists of 3 phases.
- PRICE protocol within first 24 hrs of injury.
- Motion and strength exercises starting within 48-72 hours of injury.
- Endurance training and training to improve balance after second phase begins.
References:
1. Handel DA, Gaines S. Ankle Injuries. In: Tintinalli JE, Stapczynski J, Ma O, Yealy DM, Meckler GD, Cline DM. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e. New York, NY: McGraw-Hill; 2016.
2. Tiemstra, JD. Update on Acute Ankle Sprains. American Family Physician. 2012;85(12):1170–1176.