The Basics of Bell's
Bell’s Palsy is the term commonly used for acute cranial nerve VII aka Facial nerve, paralysis of undetermined cause. It represents about ½ of all facial nerve paralysis and has an annual incidence of 13-34 cases per 100,000. Most believe that Bell’s Palsy is caused by a viral infection, most likely HSV or VZV, however it has been associated with Lyme disease as well. Recognizing this is important as it has serious mimickers such as acute ischemic stroke, TIA, and hemorrhagic stroke.

Clinical features:
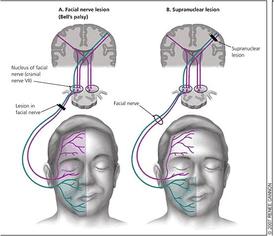
Patients will have acute onset of unilateral facial weakness, notably facial droop, loss of nasolabial fold, inability to close the affected side eye, and inability to raise the affected side eyebrow (which helps distinguish this as a peripheral palsy and not a central cause.)
Treatment:
Treatment involves glucocorticoids +/- antivirals along with eye protection. If the onset is less than 48-72 hours, treatment is indicated. There is a grading scale for severity called the House-Brackmann classification,
which can be found here. In all cases, recommended treatment within 3 days of onset is prednisone 60-80mg/day x1 week. In severe cases (House-Brackmann class IV or V), add valacyclovir 1000mg TID x1 week. Unless Lyme disease is highly suspected, there is no indication for treatment with doxycycline, which has limited effect on facial nerve palsy anyway, but is good for reducing systemic effects. All patients should be prescribed artificial tears along with eye protection during the day and an eye patch at night to protect corneal abrasions.
Resources:
Ronthal, M: Bell's palsy: Pathogenesis, clinical features, and diagnosis in adults. In: UpToDate, Shefner, JM (Ed), Dashe, JF (Ed), UpToDate, Waltham, MA, 2017
Ronthal, M: Bell's palsy: Treatment and prognosis in adults. In: UpToDate, Shefner, JM (Ed), Dashe, JF (Ed), UpToDate, Waltham, MA, 2017
Image from: https://manumissio.wikispaces.com/Facial+Paralysis+(Bell%27s+Palsy), accessed online June 29, 2017