Biliary Disease
Thu, 04/29/2021 - 6:00am
Editor:
Signs:
- Murphy’s sign: When palpating RUQ, have patient take deep breath simultaneously; Positive sign = cessation of inspiration secondary to pain
- Sonographic Murphy’s: Maximal abdominal tenderness from pressure of the US probe over the visualized gallbladder; Does not have to do with inspiration!
- Courvoisier’s signs: Palpable gallbladder on jaundiced patient
- Porcelain Gallbladder: Calcification of galldbladder thought to be related to chronic cholecystitis; correlated with increased rate of malignancy
Biliary Colic:
- Pathophysiology: pain is due to increased luminal pressure from obstructed gallbladder neck or cystic duct due to stone or sludge
- Clinical:
- RUQ, epigastric, substernal pain
- Pain can radiate to back or right shoulder
- Pain is constant despite the name of colic
- Associated Nausea, Vomiting & Diarrhea
- Gradually resolve after < 6 hours so by the time we them, patient may be pain free; peak pain severity is about 1 hour
- Why are Gallstones so Important: because of the complications they cause!
- Cholecystitis
- Choledocholithiasis
- Acute Cholangitis
- Gallstone Pancreatitis
- Gallstone Ileus
- Mirizzi Syndrome: Stone impocated in neck or distal cytic duct that is so large that it compresses the common hepatic duct.
Cholelithiasis:
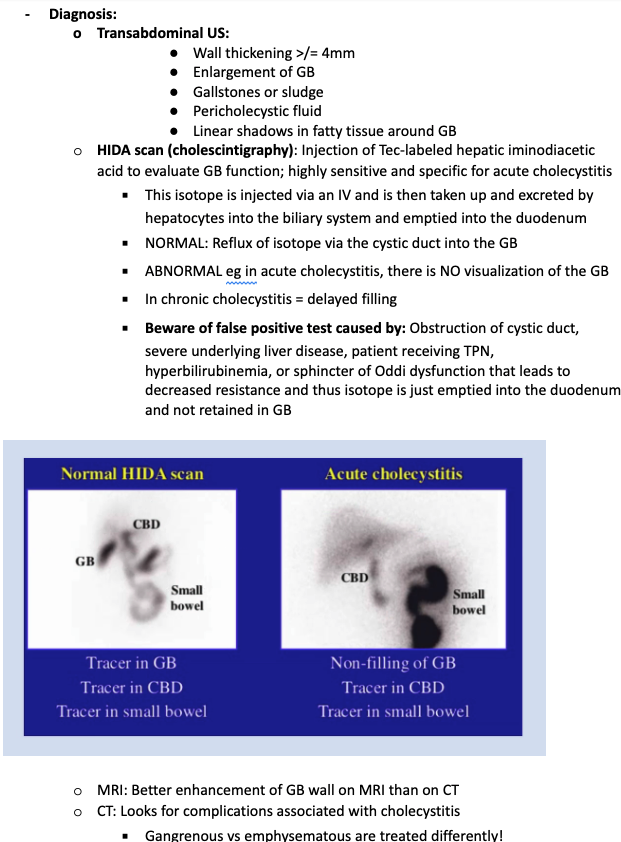
- Diagnosis:
- Transabdominal Ultrasound: sensitivity ~ 95% for detecting stones > 3 mm; sensitivty drops to ~60 if gallstones are < 3 mm
- If Transabdominal Ultrasound is negative:
- Repeat US in 1 week if high suspicion negative US (there may be a small stone
- Endoscopic US by GI is another option (indicated when pretest probability is high)
- Management:
- Analgesia: can start with an NSAID such as Toradol
- Cholecystectomy: will be needed eventually so give patient outpatient surgical referral
Cholecystitis:
- Prognostication: Tokyo Guidelines
- Provides diagnostic criteria and severity grading for Acute Cholecystitis
- Hypotensive, AMS, WBC > 18k, Platelets < 100k, INR > 1.5, Cr > 2 = SICK PATIENT
- Management:
- Analgesia, Resuscitation as needed
- Antibiotics:
- Zosyn
- Cefepime & Flagyl
- Ertapenem
- Consult: Surgery
Choledocholithiasis:
- Primary: formation of stones within Common Bile Duct (CBD)
- Etiology: Biliary Stasis, Cystic Fibrosis
- Secondary: passage of stone from Gallbladder into CBD
Acute Cholangitis