Board Review:
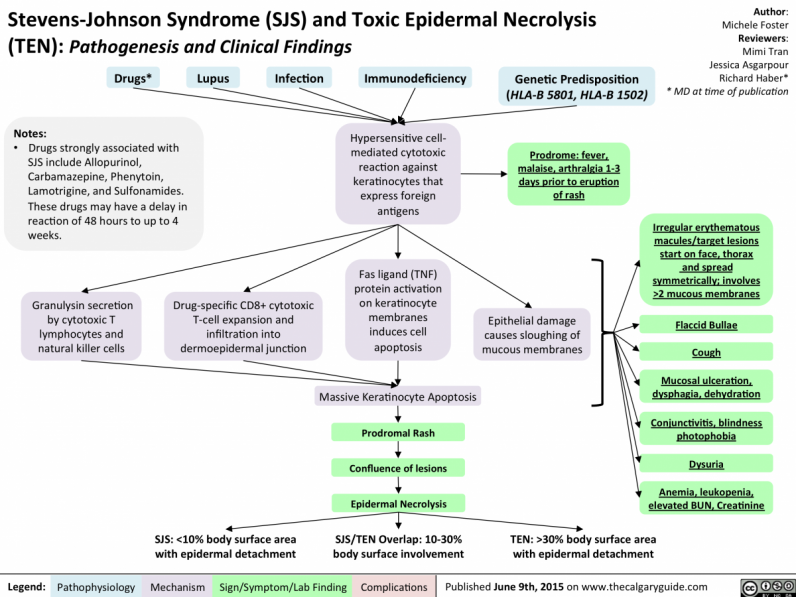
A four year old female with a history of seizures presents to the ED with a progressively worsening rash in the setting of 2 days of fever. Mom reports the rash began as diffuse erythematous maculopapular lesions exquisitely tender to touch in the face and chest, then spread to the rest of her body and evolved into blisters. Mom also noticed today that the rash involves her mouth and lips. Nikolsky sign is positive. Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) are on your differential - how would you distinguish between the two?

-
SJS has a positive Nikolsky sign; TEN does not
-
TEN has a positive Nikolsky sign; SJS does not
-
SJS involves <10% of the epidermis; TEN involves >30% of the epidermis
-
TEN involves <10% of the epidermis; SJS involves >30% of the epidermis
Answer: C. SJS/TEN is a spectrum of disease characterized by epidermal detachment usually triggered by drugs or illness. SJS is less severe compared to TEN, and both often manifest with mucosal involvement (which can include the entire GI tract and GU regions) and Nikolsky sign. Antiepileptics and sulfonamides are a common trigger in the pediatric population, as is preceding infection with mycoplasma pneumoniae. Allopurinol is another known inciting drug. This an acutely life threatening illness. Patients with SJS/TEN are at risk for hypovolemic shock, sepsis, renal failure, and airway compromise. The overall mortality rate for SJS/TEN is 30%. Consider early transfer to a burn unit.
The Calgary Guide."SJS and TEN- Pathogenesis and Clinical Findings." 9 Jun 2015<https://calgaryguide.ucalgary.ca/stevens-johnson-syndrome-sjs-and-toxic-.... 5 sept 2020.