Board Review: Acute Signs and Symptoms
You are working in a community Emergency Department overnight when you get a call from EMS that they are bringing in a family that was involved in an MVC. The first patient that arrives is a six-year-old male that was unrestrained in the front seat. GCS 3. You are preparing to intubate and obtain IV access. On your first three passes you are unable to visualize the vocal cords secondary to heavy bleeding and deformity in the airway. Oxygen saturation is 70% and you attempt to bag the patient with no improvement. What equipment should you grab next?
A. Scalpel, bougie, 4-0 ET tube
B. Glidescope or CMAC with hyper-angulated blade
C. 14 gauge needle, 3cc syringe, 7-0 ET tube adapter
D. Supraglottic airway
E. Intubating bronchoscope
Answer: C. 14 gauge needle, 3cc syringe, 7-0 ET tube adapter
Pediatric patients with significant airway trauma may require jet ventilation. This is not a definitive airway but a bridge until an airway can be established. In a community setting this will provide extra time for further equipment or anesthesia to arrive at the bedside. It is important to know the proper equipment prior to an emergency situation as these are typically performed in crash situations. You will need:
· A 16 gauge or bigger catheter
· 3mL syringe
· Connective tubing for high pressure oxygenation
· Adapter to 7-0 ETT
· BVM
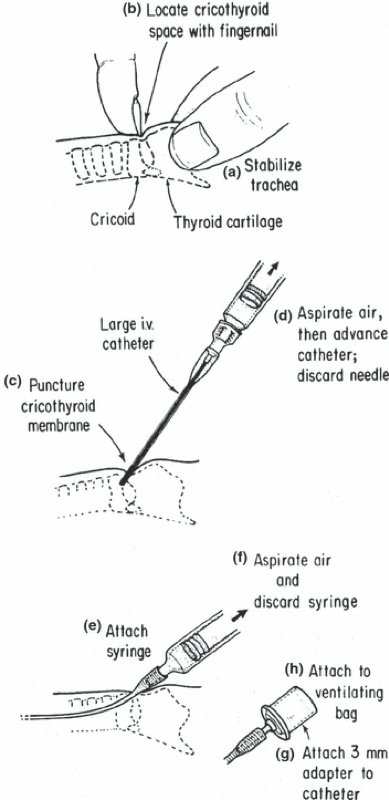
Clean the side with iodine solution. Apply sterile gloves. Connect needle onto 3 cc syringe and palpate the cricothyroid membrane. Insert at forty-five-degree angle caudally while aspirating. Once you obtain air in the syringe advance the catheter over the needle. At this point you have two option. The first is to attach a 3-0 ETT adaptor directly to the catheter. The second is to attach 3mL syringe to catheter and 7-0 ETT adapter to the syringe. You can then start bagging while setting up high flow ventilation. Respiratory therapy should be able to assist you in this portion. The goal is to pressured oxygen at a psi of around 50. Once again, this is not a definitive airway but can provide oxygenation while an airway is obtained. The maximum amount of time it should be used for is approximately forty minutes.
Resources:
Coté, C. J., & Hartnick, C. J. (2009). Pediatric transtracheal and cricothyrotomy airway devices for emergency use: which are appropriate for infants and children?. Paediatric anaesthesia, 19 Suppl 1, 66–76. https://doi.org/10.1111/j.1460-9592.2009.02996.x
Mace, S. (2008). Needle cricothyrotomy. Emergency Medicine Clinics of North America., 26(4), 1085–101, xi. https://doi.org/10.1016/j.emc.2008.09.004
Smith, M. D., & Yealy, D. M. (2016). Section 4: Resuscitative Procedures. In Tintinalli's emergency medicine: A comprehensive study guide (8th ed., pp. 192-197). New York, NY: Mc Graw-Hill Education.