Board Review: Are we seeing eye to eye?
A 65 year old female with a history of hyperopia presents to the ED with acute onset unilateral eye pain, redness, and blurry vision associated with headache and nausea. She had just arrived at a movie theater when the symptoms began. On exam you see conjunctival injection, mid-fixed pupil, and a hazy cornea. IOP of the affected eye is 40 mmHg. Topical anesthetic applied to the eye provides no significant pain relief. Treatments for this condition include all of the following except:
A. Pilocarpine
B. Timolol
C. Acetazolamide
D. Tobramycin
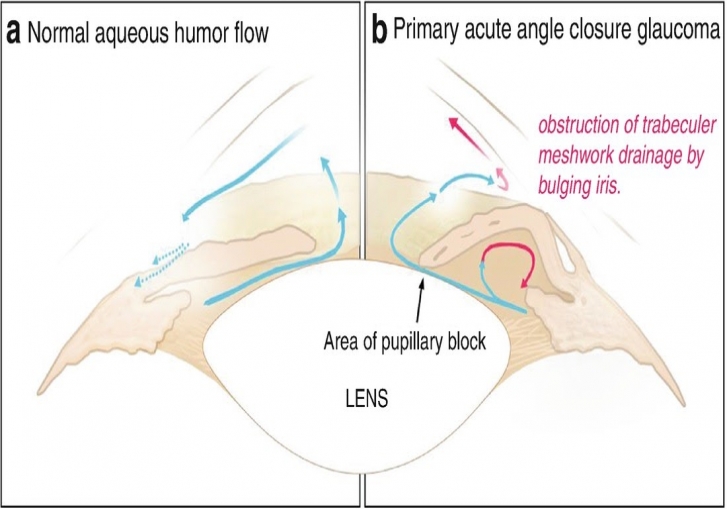
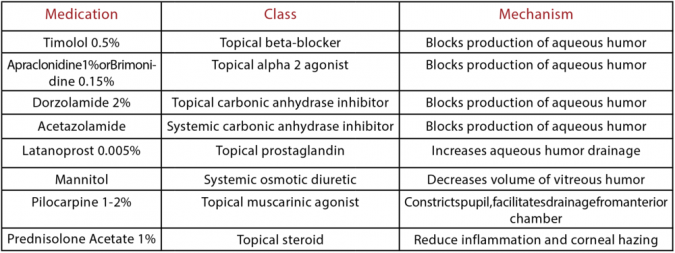
Answer: D. This patient’s presentation is consistent with acute angle closure glaucoma. In this condition, the anterior chamber angle becomes narrowed, blocking aqueous humor outflow and resulting in increased IOP > 21 mmHg that ultimately damages the optic nerve. Pilocarpine is a parasympathomimetic that facilitates aqueous humor outflow. Timolol, a beta blocker, reduces aqueous humor production. Acetazolamide inhibits aqueous humor secretion. Antibiotics are not warranted. Call ophthalmology and keep the patient in a well-lit room to avoid mydriasis that will further narrow the angle!
Williams D. (2018) Acute Angle-Closure Glaucoma. In: Long B., Koyfman A. (eds) Handbook of Emergency Ophthalmology. Springer, Cham
http://www.tamingthesru.com/blog/annals-of-b-pod/b-pod-case/angle-closur...