Board Review: In from one END out the OTHER
A 60 yo female with a history of DM and HTN presents to the ED with fever and AMS. Family reports that this morning she appeared confused and generally ill, prompting a call to 911. In the ED, her vital signs are as follows: T: 39C; HR:120; BP: 85/40; RR:26; SpO2: 97%. On exam you notice that she appears jaundiced and is exquisitely tender to palpation in the RUQ. You perform a bedside POCUS and note a dilated CBD. In addition to your resuscitation in the ED, what intervention does this patient most likely require?
A. Cholecystectomy
B. ERCP
C. Exploratory Laparotomy
D. IR Hepatic Embolization
Answer: B. This patient has Reynold’s pentad of ascending cholangitis: fever, RUQ pain, jaundice, shock, and AMS stemming from an acutely life threatening bacterial infection of the biliary system. The US image reveals a dilated CBD concerning for biliary obstruction and stasis. CT imaging will also be helpful to determine the source of biliary obstruction. In the ED, you will resuscitate this patient for septic shock including antibiotics to cover gram negative organisms but ultimately, ERCP is both diagnostic and therapeutic. Fun fact: elevation in GGT and alkaline phosphatase is 90% sensitive for a diagnosis of cholangitis.
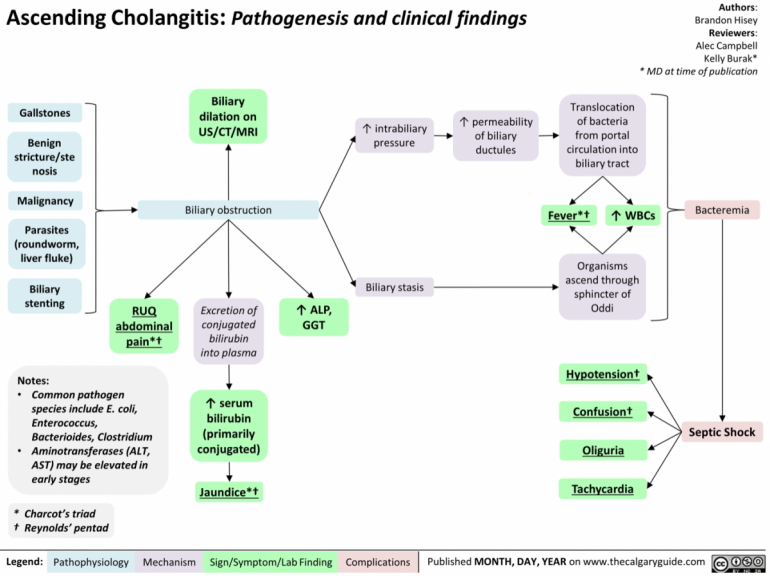
Hisey, Brandon. “Ascending Cholangitis: Pathogenesis and Clinical Findings | Calgary Guide.” Https://Calgaryguide.Ucalgary.ca/Ascending-Cholangitis-Pathogenesis-and-Clinical-Findings/, The Calgary Guide to Understanding Disease, calgaryguide.ucalgary.ca/ascending-cholangitis-pathogenesis-and-clinical-findings. Accessed 16 July 2020.