Critical Cases - Hyperkalemia Emergency!
HPI: 56 y.o. male with PMH ESRD, DM, HTN, presents with AMS and High Blood Sugar at triage and confusion
- Pt c/o diffuse abdominal pain
- States last dialysis 3 days ago
- Denies CP, SOB, N/V
Physical exam: Vitals: BP 183/78, Pulse 90, Temp 97.8 °F (36.6 °C) (Oral), RR 8, SpO2 100%
- General appearance: lethargic mainly mumbling and shakes head yes or no inconsistently
- Resp: Tachypnea, CTA b/l
- Cardiac: Tachycardic
- Abd: generalized tenderness without guarding or rebound
- Neuro: MAE equally with equal strength with poor cooperation in exam
- Skin: RUE dialysis fistula with strong palpable thrill
DDx:
- AMS secondary to DKA/HHS
- uremic encephalopathy
- hypertensive encephalopathy
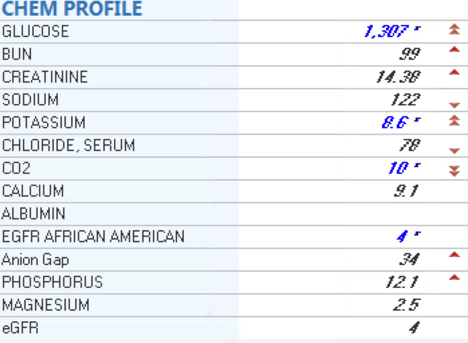
Initial workup:
- FSBS: >600
- BMP below
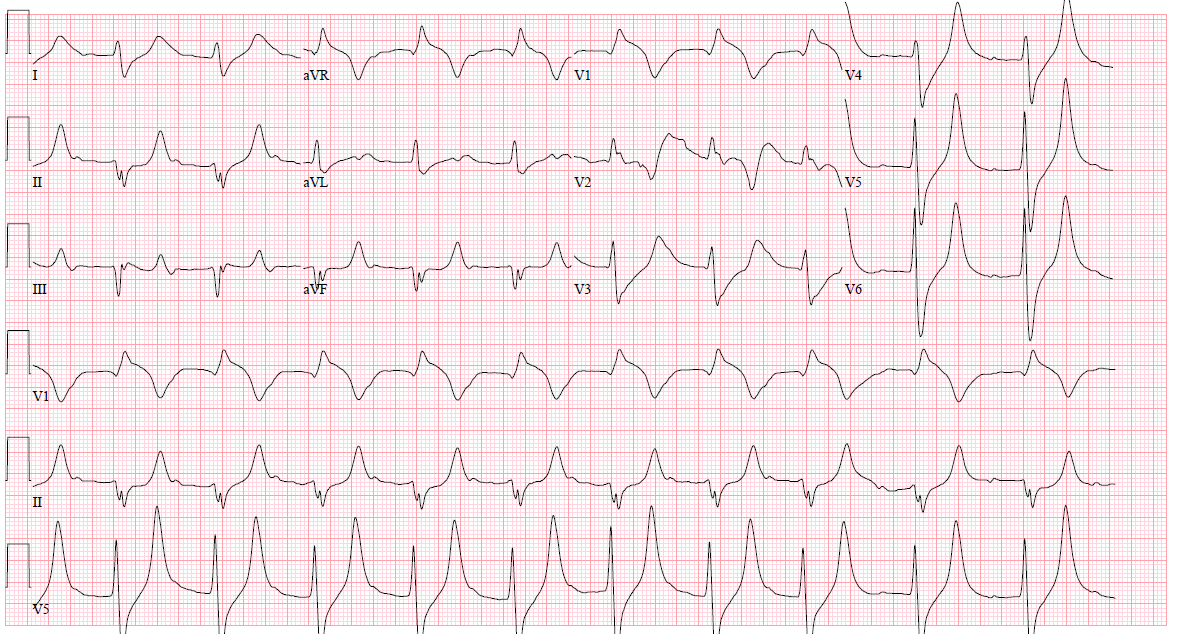
Initial EKG below at 0204, followed by repeat EKG at 0307 after MD evaluation
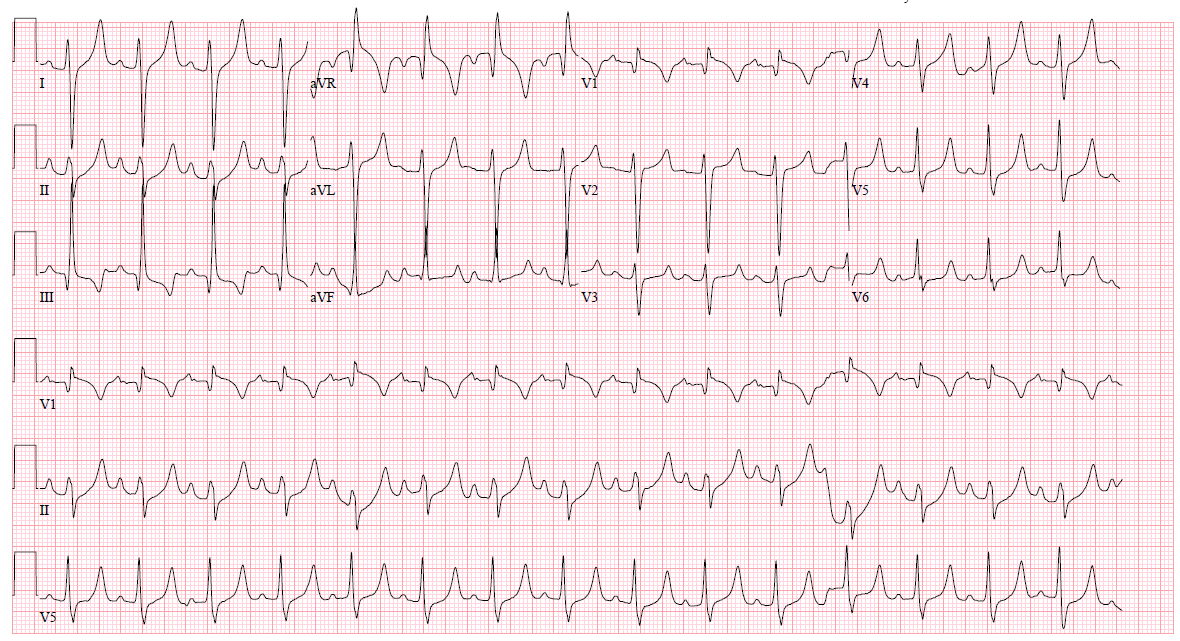
First EKG at 0204: peaked T waves, normal PR interval, normal QRS duration, P waves present
Second EKG at 0307: more severely-peaked T waves, wide QRS, absent P waves, not quite sine wave but concerning in V1
Hyperkalemia general management options:
1. Stabilize cardiac membrane:
- Calcium gluconate 10% solution: can give peripherally; 1g (10mL) over 2-3 min, repeat q5min PRN for continued EKG changes, and then repeat every 30-40 min while waiting for definitive treatment
- Calcium chloride 10% solution: ONLY via central line, 500-1000mg (5-10mL) over 2-3 minutes, repeat q5min and then repeat every 30-40 min while waiting for definitive treatment
2. Lower extracellular potassium:
- Regular insulin 10 Units IV push followed by 50 mL of D50 IV push if glucose is below 250 mg/dL. Glucose measurements q30 min due to large risk for hypoglycemia
- Albuterol: 10 to 20 mg in 4 mL of saline by nebulization over 10 minutes, repeat PRN, often do continuous neb until ekg is normal or definitive treatment Highest dose for longest duration that you have available
- Furosemide if normal renal function and not hypovolemic with max dose of 40mg IV per dose
3. Potassium elimination - definitive therapy
- Renal replacement therapy is definitive therapy; consult nephrology for emergent HD in any patient with hyperkalemia and ECG changes
- GI cation exchange resins: sodium polystyrene sulfonate, patiromer
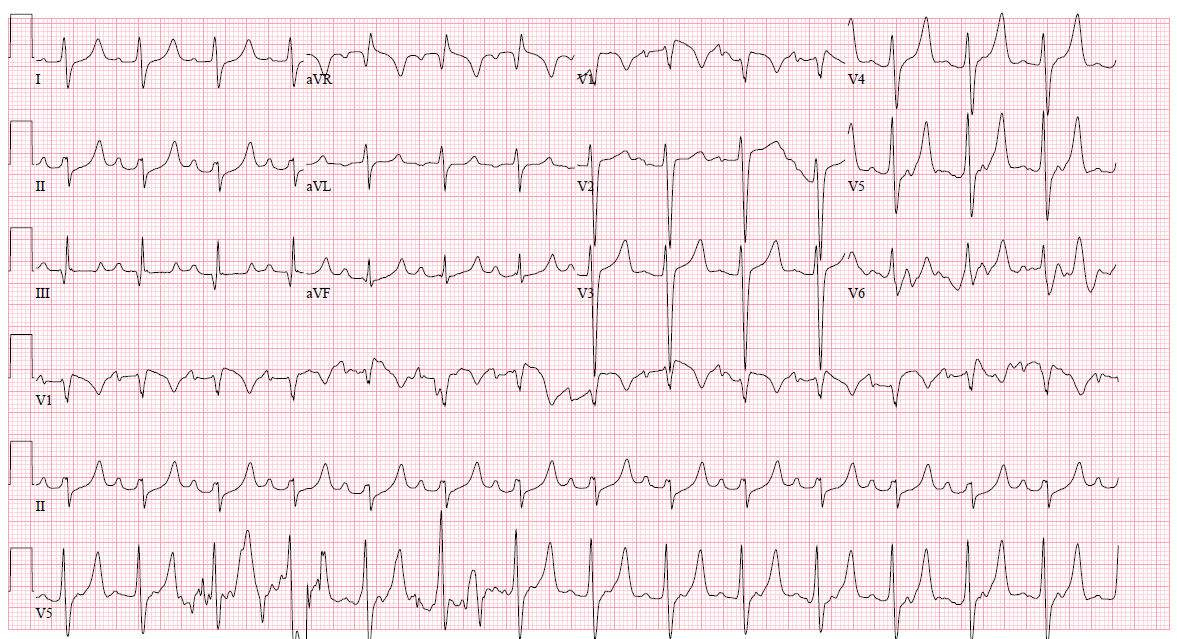
Third EKG at 0326 (after calcium gluconate, continuous albuterol neb, and 10 units of insulin IV) below
Take home points:
1. ECG changes have a low sensitivity in diagnosis of hyperkalemia
2. Treat with IV calcium early if suspected hyperkalemia while waiting for serum chemistry
References:
Montague BT, Ouellette JR, Buller GK: Retrospective review of the frequency of ECG changes in hyperkalemia. Clin J Am Soc Nephrol 2008; 3:324–330.
Weisberg LS: Management of severe hyperkalemia. Crit Care Med 2008; 36(12):3246-3251. Mount DB. Disorders of potassium balance. In: Brenner and Rector's The Kidney, 10th ed, W.B. Saunders & Company, Philadelphia 2015. P.559.
Pergola PE, DeFronzo R. Clinical disorders of hyperkalemia. In: The Kidney: Physiology and Pathophysiology, Seldin DW, Giebisch G (Eds), Lippincott Williams & Wilkins, 2000. Vol 2, p.1647. Allon M, Copkney C. Albuterol and insulin for treatment of hyperkalemia in hemodialysis patients. Kidney Int 1990; 38:869.