Critical Cases - Hypertensive Encephalopathy!
Tue, 11/17/2020 - 5:11am
Editor:
History
- 73 yo M PMH HTN, prior posterior CVA with residual peripheral vision deficit, DM, hyperlipidemia, p/w change in mental status
- Wife heard pt fall, found him down
- Immediately after the fall, patient was speaking but confused.
- Per EMS, he has had declining mental status while en route to the hospital.
- Stroke alert was called in the field by EMS
Physical Exam
T 98.4, HR 117, BP 270/143, Pulse ox 92% RA, RR 16
- Laying on stretcher with eyes closed
- Pupils equal, round, reactive, no gaze deviation
- No verbal response, not following commands
- Localizes to pain with deep sternal rub
- Cardiopulmonary exam wnl
- Abdomen soft, non-tender
Differential Diagnosis
- Stroke vs intracranial hemorrhage vs seizure
- Hypertensive encephalopathy vs PRES given marked elevation in BP
Management
- Stroke alert activated
- Pt brought to CT scanner from ambulance triage for CT head non contrast and CTA head and neck
Diagnostics and Case Progression
- CT head showed no ICH, CTA showed no LVO N
- On return from CT scan, repeat blood pressure again 270s/140s
- Symptoms suspected due to hypertension vs PRES, so nicardipine infusion was started
- As patient’s BP came down, his exam improved
- Over the next 2 hours, his systolic BP was lowered to about 200 systolic
- Repeat physical exam at this time showed patient tracking examiner with eyes and following commands in all four extremities
Discussion
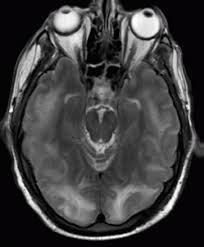
- Hypertensive encephalopthy is thought to be due to failure of cerebral autoregulation, leading to vasogenic edema especially of the posterior circulation (i.e. PRES syndrome - Posterior Reversible Encephalopathy Syndrome)
- Diagnosis suspected with acute onset encephalopathy, markedly elevated blood pressure usually >200 systolic/120 diastolic, and lack of other diagnosis to explain symptoms
- An MRI of the brain may reveal the classic changes of PRES in the posterior circulation as seen below
- Treatment is directed at reversal of underlying cause, if any, as well as reduction of systemic blood pressure with medications such as nicardepene, a peripherally acting calcium channel blocker
Reference
Feske, Steven. Posterior Reversible Encephalopathy Syndrome: A Review. Semin Neurol 2011; 31(2): 202-215.