Critical Cases: Not Just an Ankle Sprain! Demystifying the Maisonneuve Fracture
Tue, 10/19/2021 - 9:30pm
Editor:
- 0715: A patient arrives in the ED complaining of medial ankle pain after twisting it stepping off a curb
- 0730: The over-confident senior EM resident (perhaps the the author of this post about 10 years ago) orders plain films and interprets them as "no fracture"


- 0745: The patient politely inquires why, if it is only a sprain, can he dislocate and relocate his ankle? (and then demonstrates as much)
- 0750: The astute attending sends the patient back for another plain film:
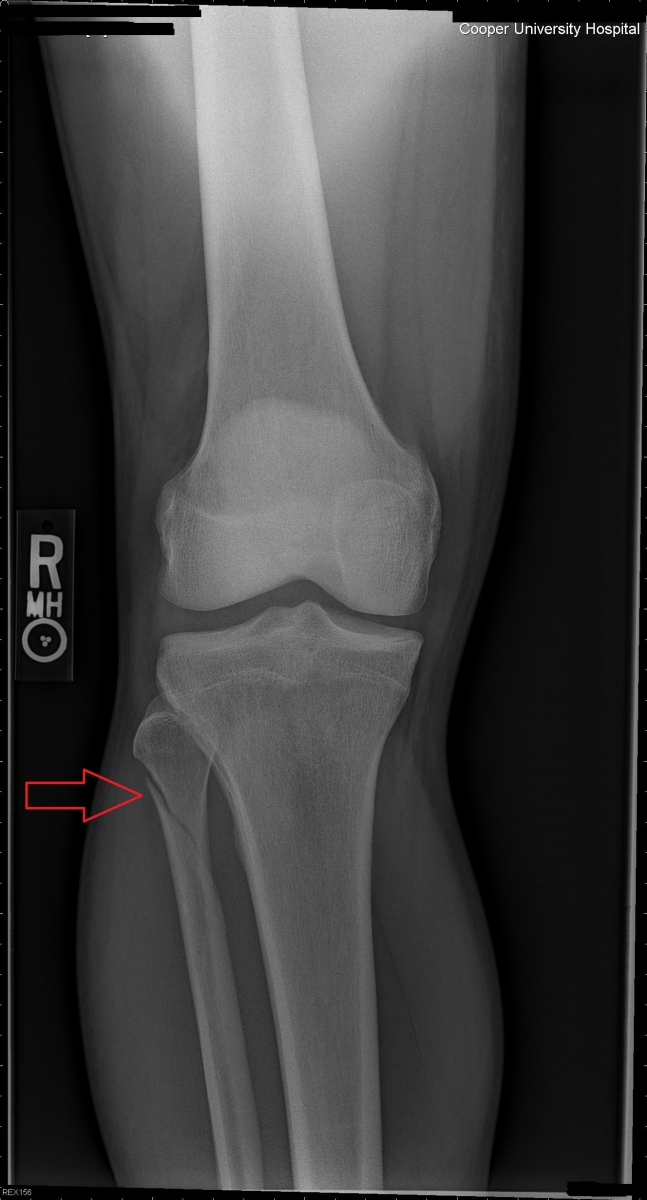
- The red arrow denotes the proximal fibular fracture that clinches the diagnosis of a Maisonneuve injury
- What was missed on the initial ankle films? Take another look at the mortise view:
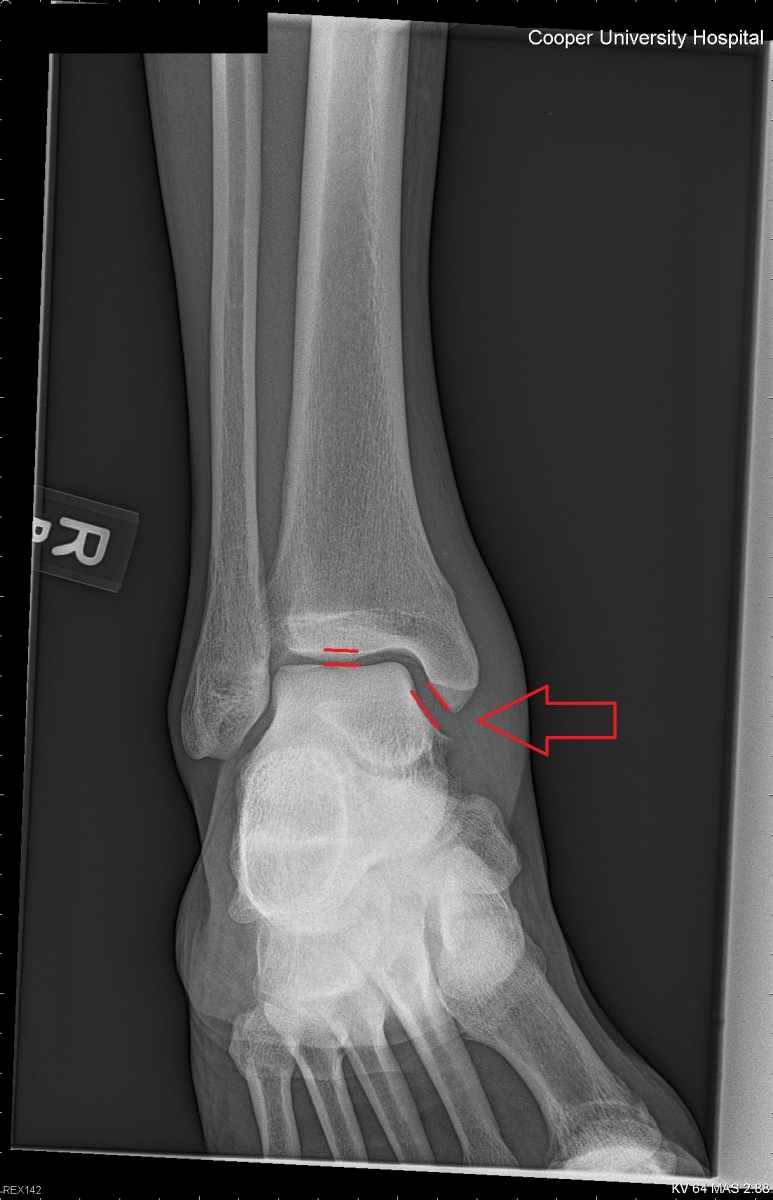
- The mortise view, obtained in a standard 3 view film of the ankle, is designed to view the entire ankle joint. As a rule of thumb, the joint space should be about the same width all the way across the tibiotalar junction. Note the slight widening medially, implying a disruption of the deltoid ligament.
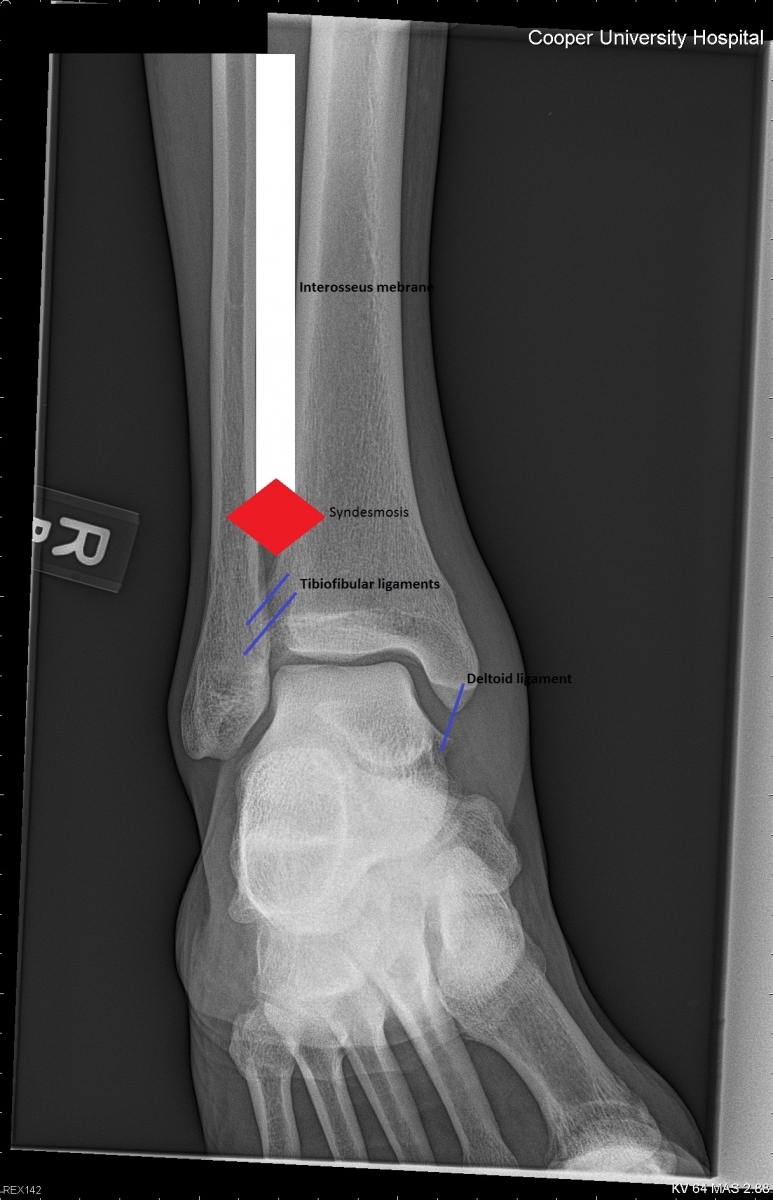
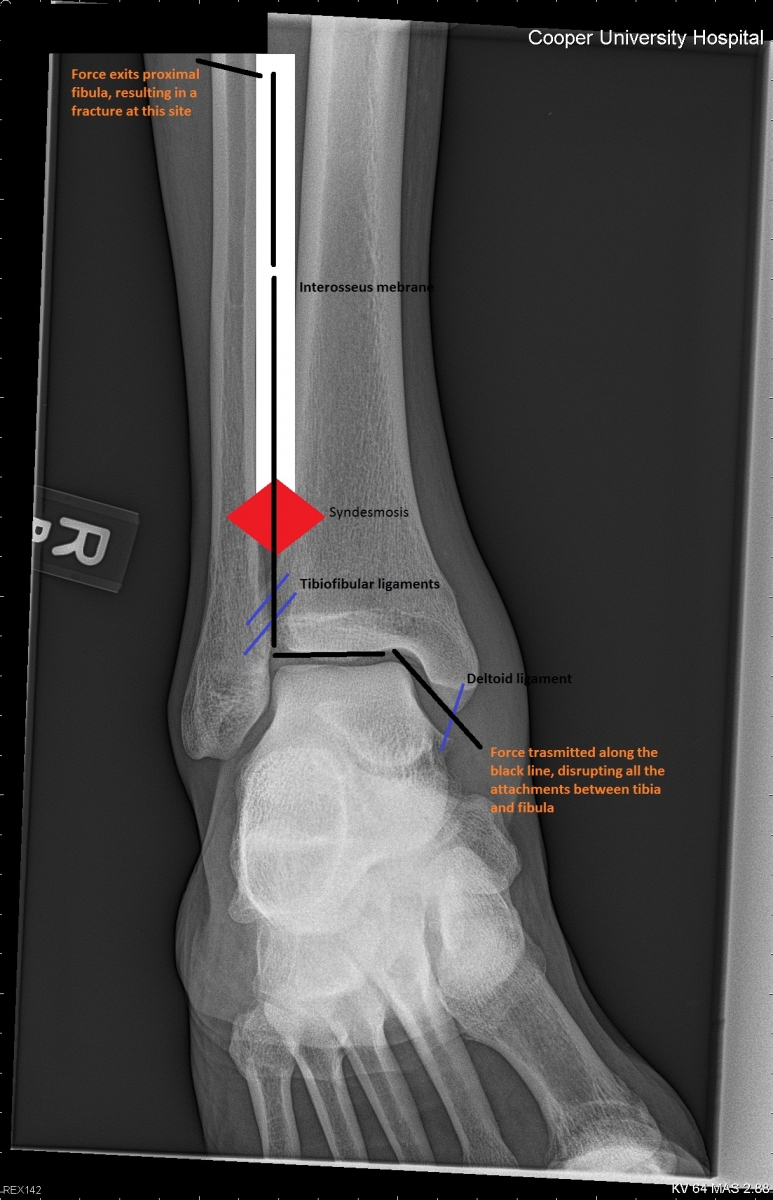
- This injury is highly unstable. Essentially all the ligaments and fascia holding the tibia and fibula together are disrupted i.e. nothing is holding your leg bones together!
- The Maissonneuve injury is very easy to miss and can result in significant morbidity if not promptly diagnosed, immobilized, and referred for surgical fixation. In fact, the old ED adage “Maisonneuve is French for ‘new house,’ as in, if you miss this injury you’ll buy the patient’s lawyer a new house.”
- This injury is very easily misdiagnosed as a "bad sprain!" Consider obtaining views of the proximal leg to assess for a fibular fracture or weight bearing views of the ankle (to accentuate mortise widening) in any medial ankle injury!
- Treatment: long leg splint, non-weight bearing, and prompt referral to orthopedics for placement of syndesmotic screws
-