Critical Cases - Pericardial effusion!
Tue, 12/03/2019 - 5:00am
Editor:
HPI
49yo F c/o diffuse abd pain. Denies cp, sob +Nausea, no emesis No change in bowel habits
PMHx
- hyperthyroidism s/p RAI w/ subsequent Hypothyroidism
- RCC s/p Nephrectomy (2008)
- bipolar disorder
- chronic anemia
Physical Exam
- BP 105/59 | Pulse 68 | Temp 98.6 °F (37 °C) (Oral) | Resp 16 | SpO2 96% | BMI 36.02 kg/m²
- Morbidly obese, appears uncomfortable and chronically ill and older than stated age
- Lungs clear
- Abdomen ttp RLQ and midline/suprapubic BLE edema
Workup
- CT A/P showed no acute intra-abdominal pathology, but incidentally found to have pericardial effusion.
DDx for pericardial effusion
- Idiopathic
- malignant
- post-MI
- uremic
- autoimmune
- radiation
- infectious
- hypothyroidism
- tuberculosis
Management
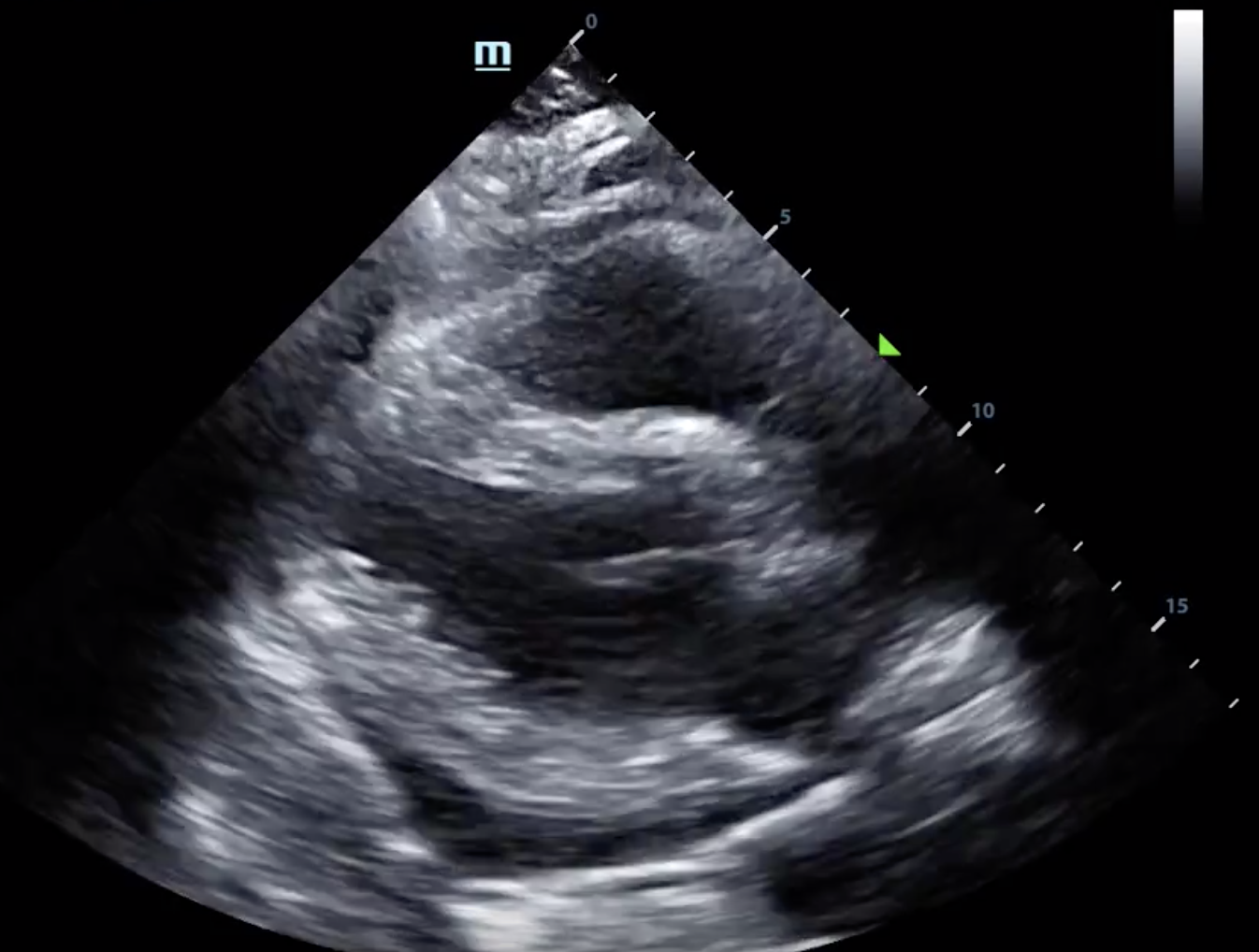
- Upon evaluation with cardiac POCUS, noted to have early tamponade physiology
- Repeat BP was 87/50
- Seen by cardiology, who admitted patient to the cardiac ICU for serial echocardiograms and continuous monitoring of vitals
- Interventional cardiology decided to defer pericardiocentesis as pt was asymptomatic and effusion was posterior and difficult to access •
- Labs showed TSH 74.6; FT4 <.1
Take Home Points
-
Remember hypothyroidism as a potential cause of pericardial effusion
- Don't forget your POCUS findings for pericardial tamponade: RV diastolic collapse, IVC dilation, hyperdynamic LV
References:
Chahine J, Ala CK, Gentry JL, et al. Pericardial diseases in patients with hypothyroidism Heart 2019;105:1027-1033.
Synovitz CK, Brown EJ. Pericardiocentesis. In: Tintinalli JE, Stapczynski J, Ma O, Yealy DM, Meckler GD, Cline DM. eds. Tintinalli’s Emergency Medicine: A Comprehensive Study Guide, 8e New York, NY: McGraw-Hill; 2016.