Critical Cases - Spontaneous pneumothorax!
History
-
25 yo male no medical history presents c/o pain to L chest and L upper back which began mid-bench press at the gym
-
Pain is sharp, pleuritic, constant
-
Pt endorses dyspnea on exertion
-
Pain is not reproducible with bending/twisting/palpation
Exam
- VS T 98.7 HR 92 BP 129/70 Pox 96% on RA
- Pt appears comfortable in no distress
- Cardiac: no murmurs/rubs, no focal tenderness over chest wall
- Pulm: diminished breath sounds on L
- Abd: soft, nontender
- Extrem: no LE edema
ECG

ECG interp: NSR, no ST/T wave changes, normal intervals. Unremarkable ECG
CXR:
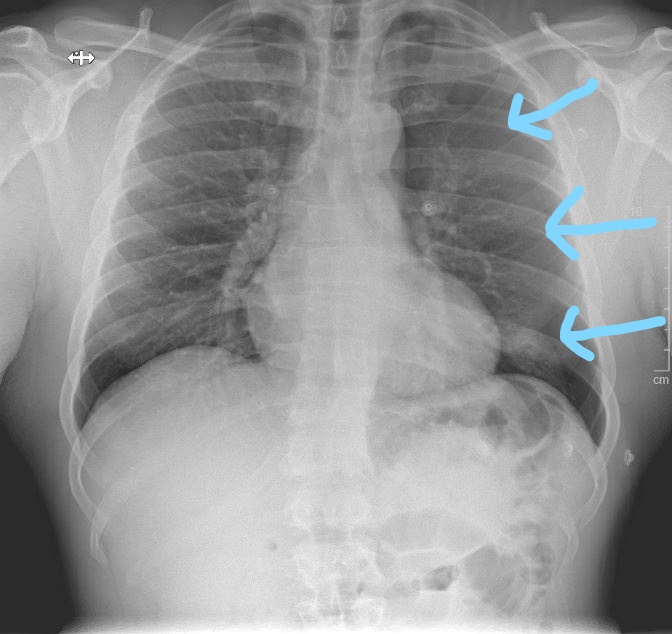
CXR interp: Moderate sized L sided pneumothorax (blue arrows show pleural line)
Management
- Options for management include observation on oxygen, aspiration, and placement of small bore chest tube
- Pt consented for placement of small-bore 14F pigtail chest tube placement
- Chest tube placed in L anterior 2nd ICS under ultrasound guidance with patient in supine position
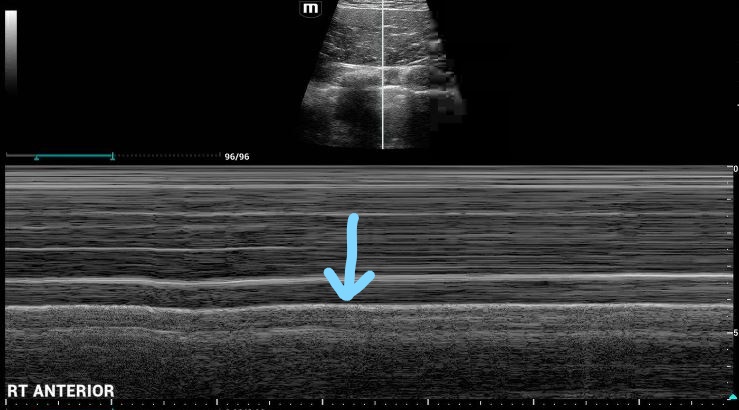
M-Mode Ultrasound Right (unaffected) lung: Interp: The blue arrow denotes the pleural line. Note the "waves on a beach" appearance below this line, indicative of lung sliding
Left lung ultrasound M-mode
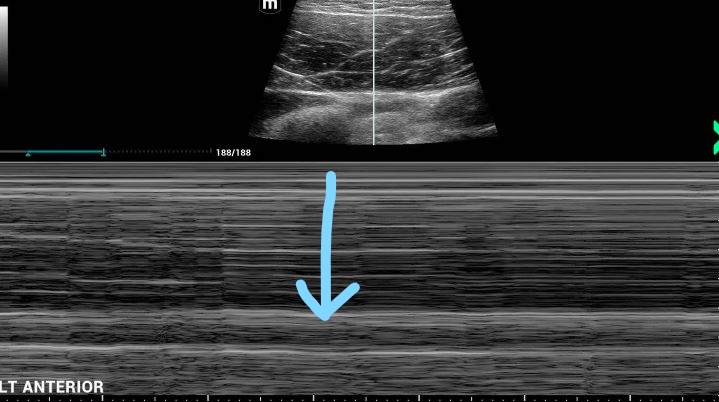
Interp: note the blue arrow again indicating the pleural line, and the "bar code" straight lines beneath this, which has the appearance of the superficial chest wall tissues above the pleural line. This indicates no lung sliding and confirms no lung is adherent to the chest wall at this site, making percutaneous chest tube placement safe
Outcome and Teaching Points
- Patient admitted with chest tube connected to low wall suction
- Remember spontaneous pneumothorax as a cause of acute chest pain in otherwise young, healthy individuals
- Classically these patients will be tall, thin, and often smokers
- A small bore chest tube or simple aspiration and observation are the treatments of choice for moderate/large pneumothorax
- Consider anterior placement with the patient in supine position: the air in the pneumothorax will rise anterior to the lung and provide the largest safe pocket to access with the seldinger technique
- Ultrasound should be utilized to ensure the absence of lung sliding in the area chosen for tube placement: this will avoid placement of pigtail into lung parenchyma, a rare but potentially serious complication