Critical Cases - Tension Pneumothorax!
Tue, 10/26/2021 - 5:26am
Editor:
History
- 76 yo F Stage IV breast Ca with metastasis to the lungs and recurrent maligant pleural effusions
- Acute onset of dyspnea which progressed rapidly
- Denies: chest pain,cough, fever, leg swelling or pain, or hx of VTE
Physical Exam
T 98.7 BP 151/72 HR 71 RR 26 Pox 84% on RA
- Pt tachypneic and anxious appearing
- No JVD noted
- Diminished breath sounds on R, clear on L
- There is a capped chest tube in the R posterior axillary position
- Heart sounds normal no murmurs
- Abd soft NTND
- No LE edema
Bedside Diagnostics
- Bedside ultrasound: no lung sliding on R side
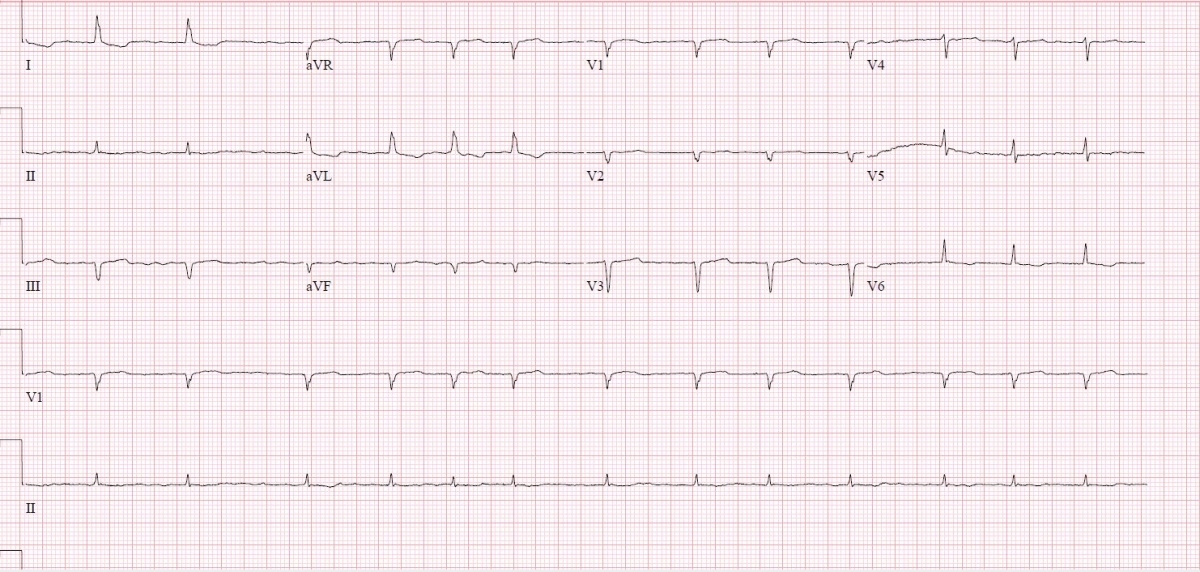
- ECG: Afib rate controlled, low voltage
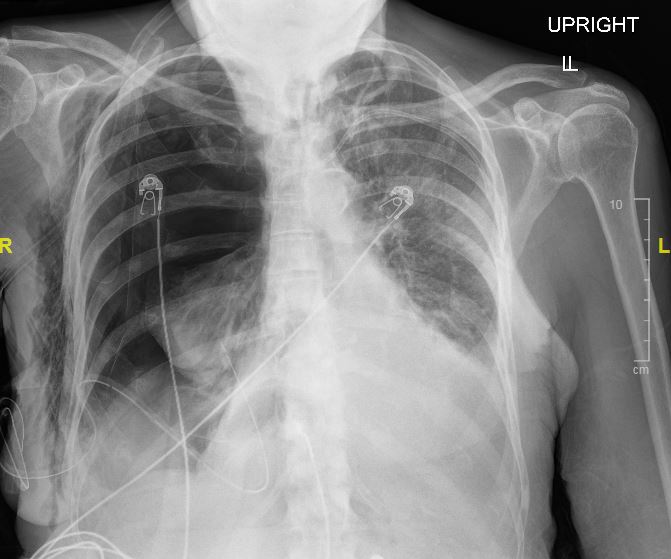
- Portable CXR: Large R sided pneumothorax with mediastinal shift to the L, R sided chest tube in place, R sided SQ air
Diagnosis
- Post-procedural tension pneumothorax
Management
- Oxygen delivered by high flow nasal canula at 30 LPM and 100% FiO2 with O2 sats increased to 98%
- 2 18 gauge IVs placed
- Given hemodynamic stability of patient, immediate needle decompression deferred and pt was discussed with interventional pulmonology
- Unfortunately, adapter for PleurX catheter not immediately available to evacuate the pneumothorax
- Decision made in conjunction with patient to place urgent R sided small bore 8F pigtail chest tube
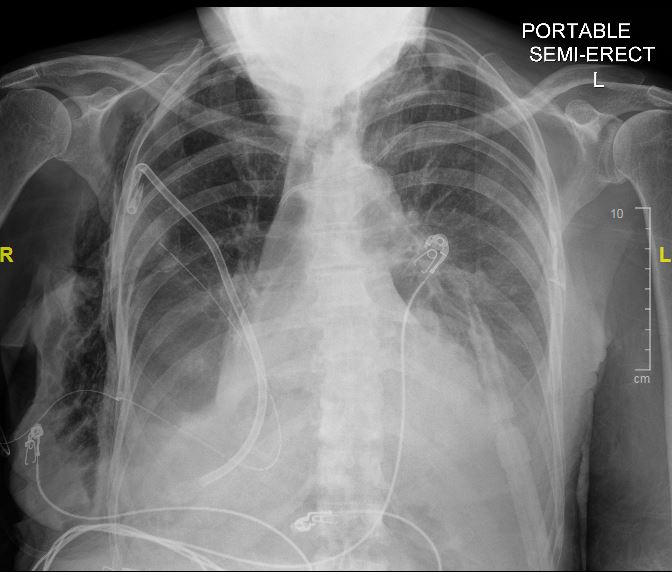
- Post-procedure chest portable CXR shows: resolution of R sided pneumothorax, mediastinal shift resolved, R sided anterior pigtail catheter in place, +R sided SQ air
- Pt quickly weaned to 2L NC, with rapid resolution of dyspnea and tachypnea
Discussion
- Tension pneumothorax (TPTX) is a rare condition which can rapidly result in hypoxemia, hypotention, and death
- It is usually diagnosed in trauma patients or patients undergoing mechanical ventilation
- The traditional signs and symptoms such as: hypotension, distended neck veins, and tracheal deviation are inconsistently present
- Traditional teaching has been to never wait for radiography to confirm the diagnosis, however a 2003 case series study of 30 ED patients found no increased mortality in hemodynamically stable patients with TPTX diagnosed on chest xray
- Indications for immediate needle decompression in patients with clincally suspected or POC ultrasound confirmed TPTX: Hypotension, hypoxemia refractory to )2 therapy, cardiac arrest, decreased level of consciousness, or RR <10
- If no indication for immediate decompression: placement of small bore chest tube, preferably in the anterior mid-clavicular 2nd intercostal space (because pleural air rises to the apical area), is the treatment of choice
- The PleurX catheter is designed for easy drainage of recurrent pleural effusions, however the adapter piece is proprietary and thus this chest tube is not easily accessed without a special kit: one option in an emergency is to cut the chest tube proximal to the drainage adapter and attach a Pleuravac directly to the tubing
Sources
Clark S et al. Is Mediastinal Shift Always an Emergency? Emergency Medicine 2003; 15:429-433.
Leigh-Smith S, Harris T. Tension Pneumothorax, Time for a Re-think? Emerg Med J 2005; 22:8-16.