#EMConf: Facial Fractures
Thu, 03/04/2021 - 5:00am
Editor:
Orbital Fractures
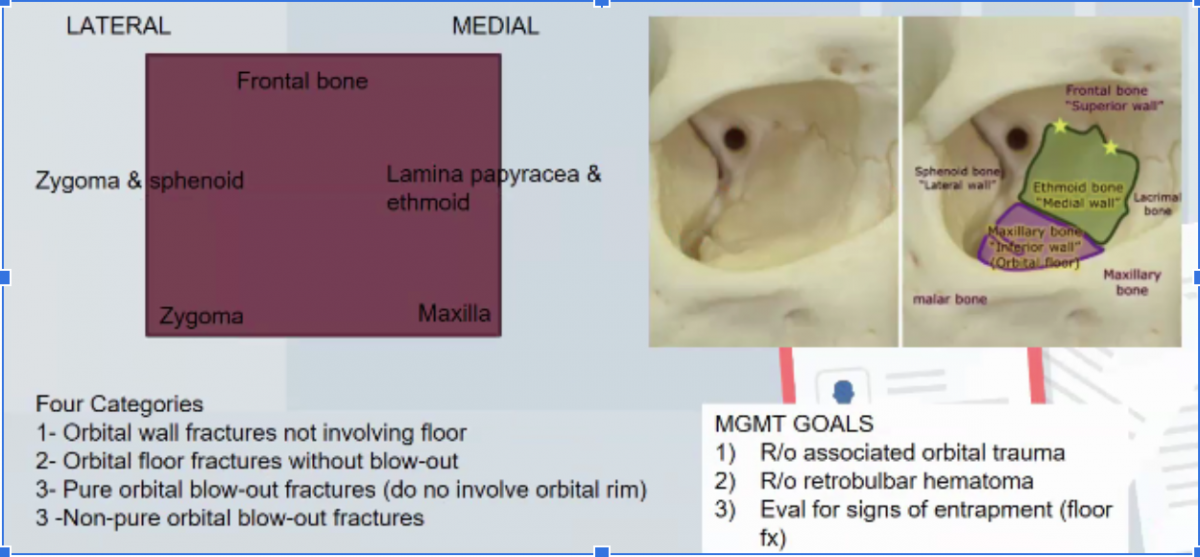 Orbital Blowout Fracture:
Orbital Blowout Fracture:
- Involves medial and inferior walls
- Need to check visual acuity and sensation, extraocular movements
- Higher risk of ocular injury compared to non-pure orbital fractures (because in non-pure, orbital rim is involved, meaning the rim is taking some of the impact, vs. pure blowout, the eyeball itself is taking most of the impact, causing the wall/floor fractures)
- Always evaluate for retrobulbar hematoma!! Evaluate for proptosis, decreased visual acuity, elevated intraocular pressure (concerned if >40mmHg), afferent pupillary defect
- *Management = lateral canthotomy
Entrapment: Limitation of upward gaze from entrapment of inferior rectus muscle, binocular diplopia (vs monocular diplopia suggests lens dislocation); can have infraorbital anesthesia.
Management of Orbital Fractures:
- PO amox-clav (Augmentin) to treat sinus pathogens
- Decongestants
- Avoid nose blowing
- Facial consult before discharge
Naso-orbito-ethmoid fractures: Usually require admission and facial surgery, sometimes neurosurgery consult because they are often accompanied by injury to lacrimal duct, dural tears, and traumatic brain injury
Tripod fracture: Zygomaticomaxillary tripod fracture (malar flattening of cheek)
- Zygomatic arch
- Maxilla (including sinuses)
- Lateral orbit
LeFort Fractures: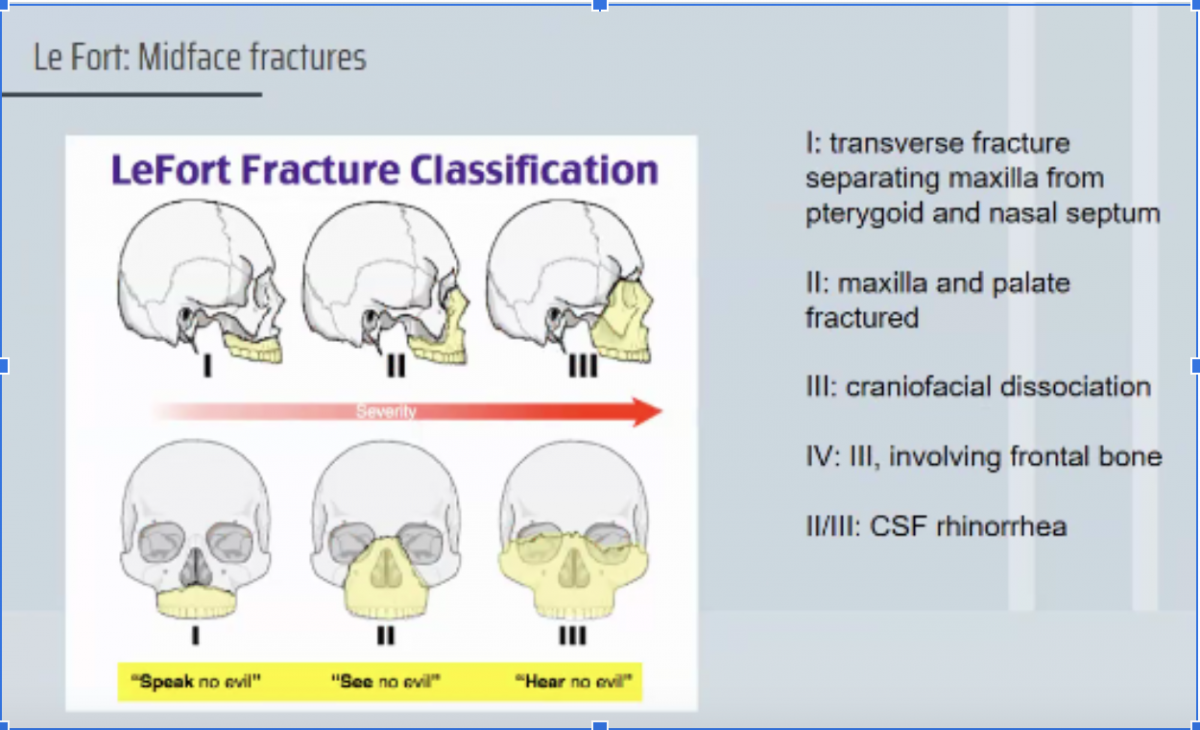
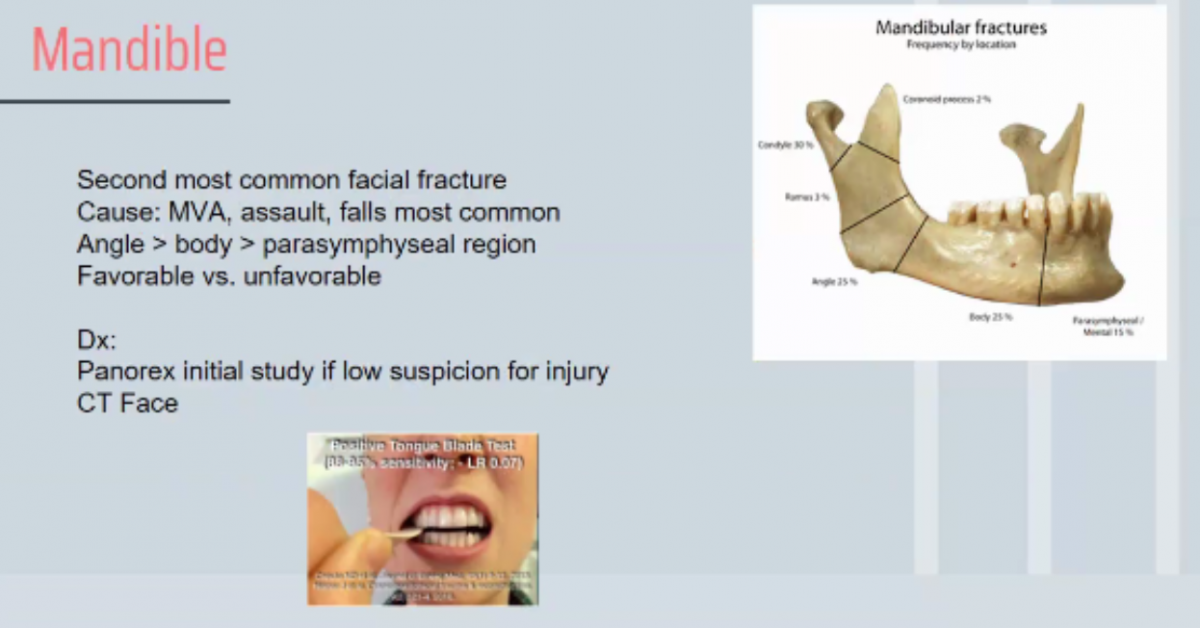
Mandibular Fractures:
- Management: All except isolated coronoid fracture will need repair, but not necessarily emergent
- Closed fracture: nondisplaced; soft/liquid diet with urgent outpatient follow up
- Open fractures: emergent consult, antibiotics (penicillin G, clindamycin), admit