Immune Checkpoint Blockade
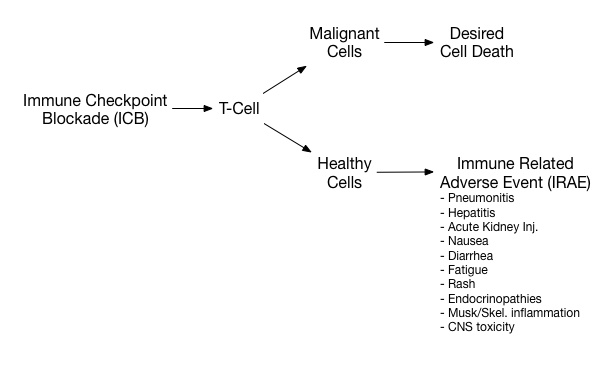
Increasingly, patients are taking immune checkpoint blockade (ICB) therapy to restore their T-cell immunity against malignant cells. These therapies have led to improved duration of survival but can come at the cost of T-cells attacking healthy cells and organs, causing immune-related adverse events (IRAEs). IRAEs can range from minor (such as fatigue) to life threatening (such as pulmonary toxicity with resulting ARDS).
A just published study from France notes that while the use of ICBs are increasing, emergency medicine physicians fail to identify that a patient is on an ICB as frequently as 33% of the time. Further, we are only slowly thinking of IRAE in our differential diagnoses and perhaps prematurely closing on infection or malignancy progression as the cause of the patient’s symptoms. Contacting the patient’s primary oncology team improved the rate of considering this diagnosis. The most commonly diagnosed IRAE in this cohort was diarrhea followed by fatigue and fever.
Identifying an IRAE and consulting with the patient’s oncology team is important. The primary oncologist will be able to assist in determining when therapy should be discontinued and when admission and inpatient management is warranted. The prescribed treatment for the IRAE will depend on the organ system involved and severity.
References:
-
Peyrony O, Tieghem Y, Franchitti J, et al. Immune checkpoint blockade toxicity among patients with cancer presenting to the emergency department. Emerg Med J. March 2019. doi:10.1136/emermed-2018-208091.
-
Brahmer JR, Lacchetti C, Schneider BJ, et al. Management of Immune-Related Adverse Events in Patients Treated With Immune Checkpoint Inhibitor Therapy: American Society of Clinical Oncology Clinical Practice Guideline. JCO. 2018;36(17):1714-1768. doi:10.1200/JCO.2017.77.6385.