What's the diagnosis? By Dr. Abby Renko
A 30 y.o. G5P3013 female at 7w6d gestation presented to the ED with severe lower abdominal pain for the last 3 days. The pain became so severe overnight that she had syncope a few hours prior to arrival. She denies any associated vaginal bleeding. PMH/PSH is significant for a prior ectopic pregnancy and she is s/p unilateral salpingectomy. Her abdomen is soft, with marked bilateral lower quadrant tenderness and involuntary guarding. Her vital signs are normal.
Bedside point of care ultrasound is performed and reveals the following images (shown below). What’s the diagnosis? Scroll down for answer.
Transvaginal US
![]()
Trans vaginal US - Mid uterus
![]()
Transvaginal US - Right uterus/adnexa
![]()
Answer: Ruptured Cornual (ie Interstitial) Ectopic Pregnancy
Epidemiology
-
Interstitial ectopic pregnancies account for only ~1% of all ectopic pregnancies, BUT they carry the highest maternal mortality rate of all ectopic sites (~2.5%) because they are still commonly misdiagnosed!
-
For example, our patient had what LOOKED to be a gestational sac in the uterus, but it was actually a pseudogestational sac (see mid uterus view above). Upon further investigation, we found the complex adnexal mass in addition to the intrauterine ‘sac’.
-
Since the interstitial portion of the fallopian tube can dilate pretty easily (in comparison to other portions of the tube), patients usually present with pain later than expected (typically ~8-10 weeks gestation).
-
Rupture occurs in 20-50% of cases.
Intradecidual Sign = IUP
-
Earliest marker of an IUP (can be seen usually around 4.5weeks gestation, when the HCG is at least 15000, and/or when the mean sac diameter is at least 3mm).
Mimickers of an intrauterine gestational sac?
-
Pseudogestational sac, ie ‘Pseudosac’
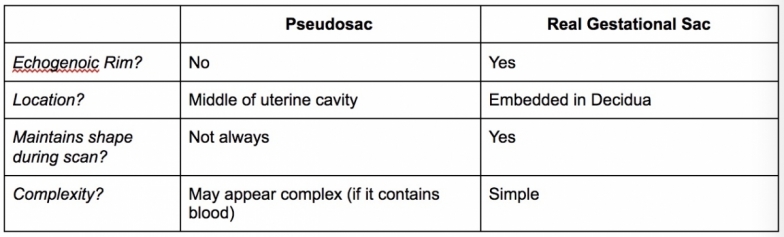
-
Decidual Cyst
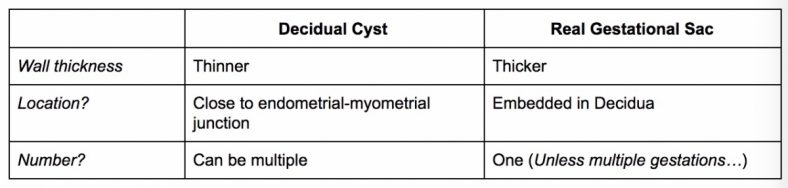
*You can have one of the above, or even (rarely) both, with an ectopic pregnancy.
Management
-
If suspected, obtain basic pre-op labs including CBC, BMP, PT/INR, Type & Screen on initial blood draw in ED. (Also, HCG quant, particularly for your OBGYN colleagues)
-
Rh-negative patients should be given Rho-GAM (anti-D immune globulin).
-
Call OBGYN as soon as your suspicion is high enough to worry about it.
References
-
Nahum GG. Rudimentary uterine horn pregnancy. The 20th-century worldwide experience of 588 cases. J Reprod Med. 2002 Feb;47(2):151-63.
-
Tulandi T, Al-Jaroudi D. Interstitial pregnancy: results generated from the Society of Reproductive Surgeons Registry. Obstet Gynecol. 2004;103(1):47.
-
Soriano D, Vicus D, Mashiach R, Schiff E, Seidman D, Goldenberg M. Laparoscopic treatment of cornual pregnancy: a series of 20 consecutive cases. Fertil Steril. 2008;90(3):839.
-
Chiang G, Levine D, Swire M, McNamara A, Mehta T. The intradecidual sign: is it reliable for diagnosis of early intrauterine pregnancy? AJR Am J Roentgenol. 2004;183(3):725.
-
Bhatt S, Ghazale H, Dogra VS. Sonographic evaluation of ectopic pregnancy. Radiol Clin North Am. 2007;45(3):549.
-
Ackerman TE, Levi CS, Lyons EA, Dashefsky SM, Lindsay DJ, Holt SC. Decidual cyst: endovaginal sonographic sign of ectopic pregnancy. Radiology. 1993;189(3):727.