What's the Diagnosis? By Dr. Abby Renko
Wed, 02/02/2022 - 12:43pm
Editor:
A 50 yo M presents to the ED w/ dental pain and facial swelling, worsening over the last 2 weeks. He denies fever, voice changes or dysphagia. On exam his temp is 99.1, HR 122 and spo2 98%. He is nontoxic appearing, has no trismus or drooling, but there is noted erythema and swelling of the L cheek down to the level of the clavicle. A CT is obtained and shown below. What's the diagnosis? (scroll down for answer)
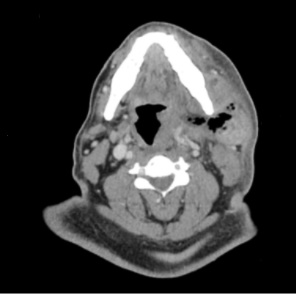
Answer: Gas producing facial cellulitis and abscess of the L masticator space (with concern for early Ludwig's angina)
- Facial space infections
- Almost always of dental origin
- Most common deep space infection= PTA
- Diagnosis you must consider in any patient w/ rapidly progressive facial/neck cellulitis-- Ludwig's Angina
- Definition
- Rapidly progressing bilateral cellulitis involving both submylohyoid and sublingual spaces, without lymphatic involvement, and generally without abscess formation
- Presentation
- Fever, chills, malaise, dental/mouth pain
- +/- stiff neck, drooling, dysphagia, voice changes
- Trismus usually absent unless infection has also spread to parapharyngeal space
- On exam:
- typically mouth held open due to lingual swelling
- palpable crepitus in submandibular space
- Diagnosis
- CT of face/neck with contrast
- Management
- Airway managment is #1 concern!
- consider glidescope, fiberoptic nasal intubation
- Antibiotics
- Unasyn 3g IV q 6h OR Ceftriaxone 2g IV q 12h + Flagyl 500mg IV q 8h
- PCN allergy: Clindamycin 600mg IV q 8 hr + Levaquin 750mg IV q 24h
- Add vancomycin for anyone w/ MRSA risk
- Early surgical consult
- Complications
- Mediastinitis
- Cavernous sinus thrombosis
References:
-
Chow, AW et al. Submandibular space infections (Ludwig’s angina). In: UpToDate, Post TW (Ed), UpToDate, Waltham, MA.
- Tintinalli, JE. Tintinalli's Emergency Medicine: A Comprehensive Study Guide. 8th ed. New York, NY: McGraw-Hill Education LLC, 2016