What's the Diagnosis? By Dr. Eric Chavis
Wed, 02/24/2021 - 3:52pm
Editor:
A 27 yo M with a PMHx of osteosarcoma s/p R hip disarticulation and numerous lung metastases s/p L upper lobe wedge resection (1 year prior) presents to ED with DOE and "abnormal findings on outpatient CT scan." On ED arrival he is tachycardic w/ HR 135, RR is 18 and SpO2 is 93% on RA. On exam he has diminished but present breath sounds bilaterally. A CXR is obtained and shown below. What's the diagnosis? (scroll down for answer)
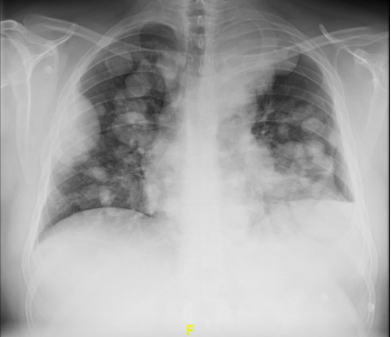
Answer: Hydropneumothorax
- Defined as the presence of both air and fluid in the pleural space
- This is indicated on CXR w/ the presence of moderate pneumothorax in addition to the air fluid level at the L base, which signifies concomitatnt pleural effusion
- Can be either atraumatic or traumatic (hemopneumothorax)
- Underlying etiologies can include: COPD (due to presence of blebs), pneumonia, TB, malignancy, prior lung instrumentation
- Most common presenting symptoms are SOB and cough
- Diagnosis can be made on CXR, US or CT
- In the event of tension physiology, treat as tension PTX w/ needle decompression, tube thoracostomy
- For more stable cases, treatment is supplemental O2 to help w lung re-expansion, tube thoracostomy and pulmonology consultation
- Ultimately, requires admission for further workup, treatment of underlying condition
- The etiology of this patient's hydropneumothorax was unknown, but possibly related to underlying malignancy
References:
Kasargod V, Awad NT. Clinical profile, etiology, and management of hydropneumothorax: An Indian experience. Lung India. 2016;33(3):278-280.