What's the diagnosis? By Dr. Katie Nowlan
A 26 yo male is brought in with a change in mental status. History from prehospital providers was limited because of language barrier between EMS and persons living in the home with the patient. Patient was regsitered with his Guatemalan ID. He was only able to state his name. He had normal vitals, and was in no distress, he had no facial droop or obvious weakness. He sat upright and stared into the distance with an odd affect, occasionally offering only one word answers to the interpreter. No additional history was available. A CT of the head is shown. What's the diagnosis? Scroll down for answer.
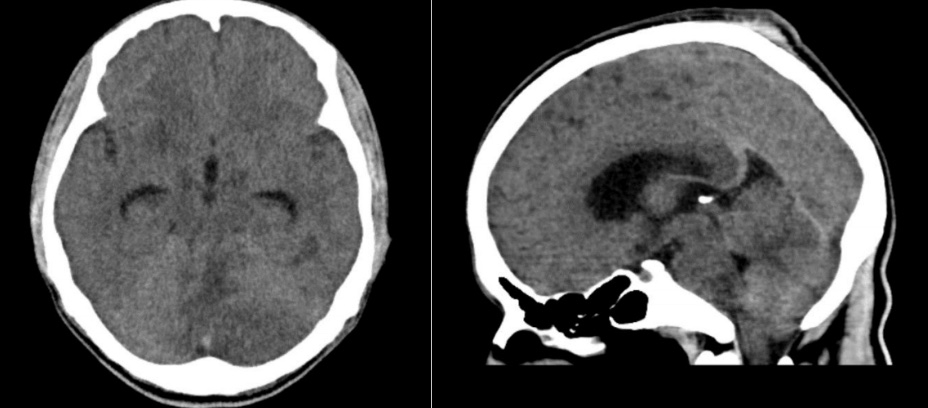
Impression
- Mild diffuse hypodensity in the left cerebellar hemisphere concerning for infarction versus neoplasm
- Slight compression of the lateral fourth ventrical
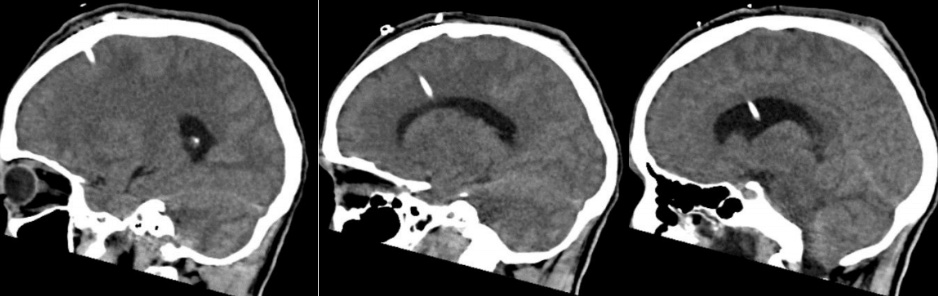
Neurology and neurosurgery called to the bedside. A bedside ventriculostomy is performed
An MRI is done to better characterize the cerebellar lesion
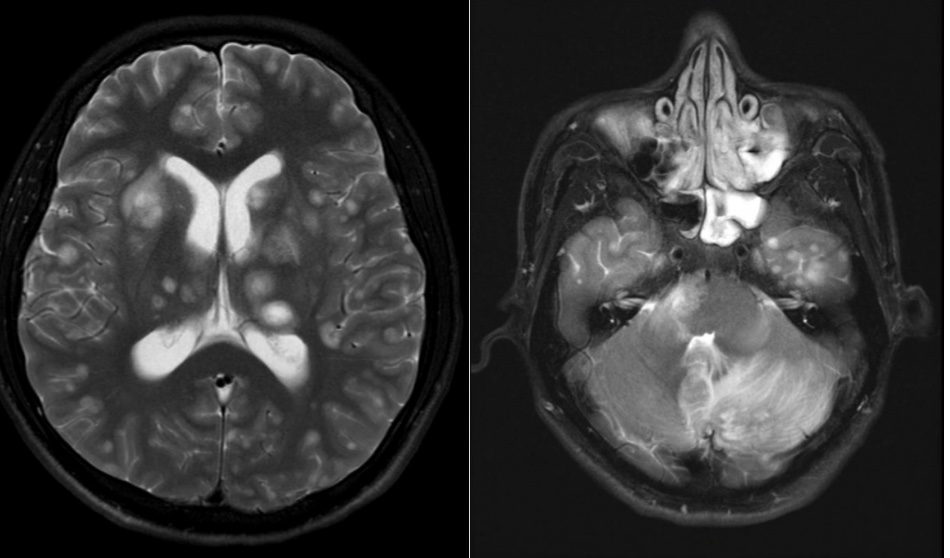
Impression: Over 100 heterogeneous ring enhancing lesions noted in bilateral hemispheres, cerebellum and pons with mild edema noted adjacent to many of these areas of foci
Hospital course:
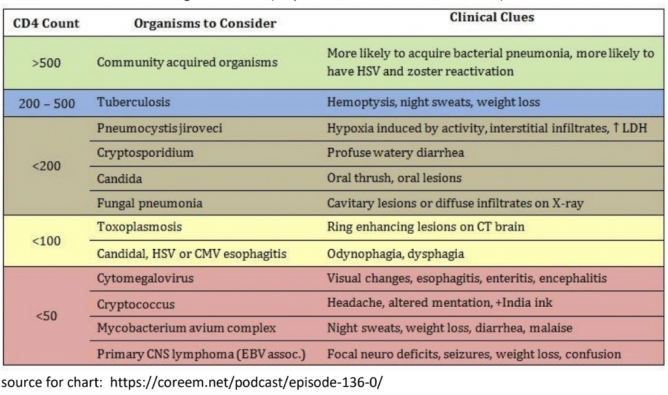
- patient had undiagnosed advanced AIDS with CD4=21 and high viral load, lesions in the brain presumed cryptococcal and toxoplasmosis infections
- patient extubated at week 3 of treatment
- pt with slight mental status improvement after 4 weeks
Teaching points
- Ventriculostomy
- normal adult ICP is 5-15 mmHg (or 7.5-20 cmH2O)
- Ventriculostomy / External ventricular drain
- gold standard for ICP monitorung and therapeutic purposes
- works like an arterial line transducer as its external transducer provides a waveform and numerical value for ICP when zeroed appropriately
- correct postion for zeroing the transducer is the level of the center of the brain which corresponds to the external auditory meatus
- if being used to drain CSF (like in this case) drains are typically left open to drain at 15 mmHG (20 cmH2O) above the ear, and then temporarily clamped once and hour to check ICP as reading is not accurate with open drain.
- AIDS
- Any new headache or new headache pattern, seizure, mental status change in patient with low CD4 warrants CT and then LP (reminder CD4<200 = AIDS)
References
Ganti L. (2016) External Ventricular Drain Placement. In: Ganti L. (eds) Atlas of Emergency MedicineProcedures. Springer, New York, NY.https://doi.org/10.1007/978-1-4939-2507-0_40
Turtz, Alan. (2008). Intracranial Monitoring. Critical Care Medicine: Principles of Diagnosis andManagement in the Adult. 281-288. 10.1016/B978-032304841-5.50019-4