What's the Diagnosis? By Erica Schramm, MD
Wed, 10/24/2018 - 9:00am
Editor:
An 80 yo F with a Pmhx of HTN, AFib and atherosclerosis presents to the ED with 1 day of severe diffuse abdominal pain, nausea and bilious vomiting. On exam she is tachycardic, and appears uncomfortable with diffuse abdominal tenderness. EKG shows rate controlled AFib. CT a/p with IV contrast is obtained. What's the diagnosis? (scroll down for answer)
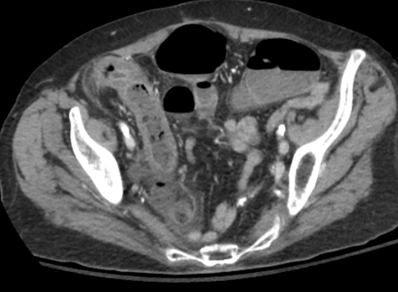
Answer: Pneumatosis intestinalis due to acute mesenteric ischemia
- Pneumatosis intestinalis is defined as gas in the bowel wall; is a radiographic finding, not a diagnosis
- Is considered an ominous finding when associated with ischemia
- Mesenteric ischemia etiology:
- Arterial
- Embolic (50%)- risk factors include Afib, MI, valvular disease, hypercoagulable state; most commonly due to SMA embolism
- Thrombosis (15-25%)- greatest risk w/ atherosclerotic disease of the mesenteric artery
- Non occlusive (15-30%)- associated w/ low arterial flow/vasoconstriction
- Venous
- Thrombosis (5%)- risk factors include portal hypertension, hypercoagulable state
- Imaging: CT vs CTA
- CT w/ IV contrast: sensitivity 64%, specificity 92%; findings include bowel wall edema, intramural gas
- CTA: considered to be imaging study of choice; sensitivity 89-96%
- Treatment includes anticoagulation, broad spectrum antibiotics, and emergent surgical consult
- Poor prognosis- survival rate 50% if diagnosed within 24 hours
References:
Lo, Bruce M. "Lower Gastrointestinal Bleeding." Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 9e Tintinalli, et al. New York, NY. McGraw-Hill, 2016.
Tavakkoli, Ali, et al. "Small Intestine." Schwartz's Principles of Surgery, 10e. F. Charles Brunicardi, et al. New York, NY. McGraw-Hill, 2015.