Critical Cases - Bradycardia Emergency!
Tue, 09/15/2020 - 5:11am
Editor:
HPI:
- 87 yo male hx of htn, afib on warfarfin, AAA s/p endovascular repair, CAD s/p CABG presents after a syncopal event on the toilet
- Pt fell and struck his head with confirmed LOC
- Wife found him down and called EMS
- Patient denies any chest pain, dyspnea, abdominal pain, nausea/vomiting, but does endorse acute onset diarrheal illness preceding the syncopal event
- Denies any recent medication changes
PE:
T 98.8 BP 154/68 HR 32 Pox 96%
- Head: +abrasion above R eye
- Neck: no c-spine tenderness
- Lungs: clear bilaterally
- Heart: bradycardic, no murmurs
- Abdomen: soft, nontender, no pulsatile masses
- Extremities: atraumatic, distal pulses intact
ECG
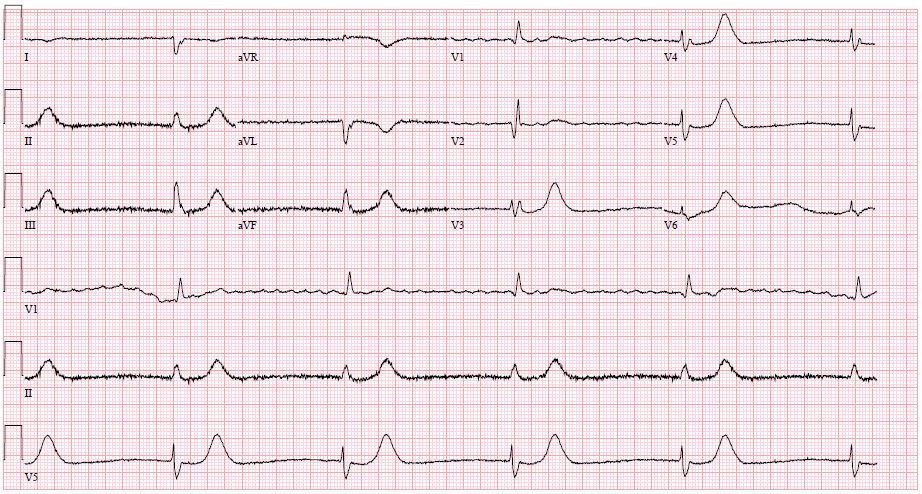
ECG Interpretation: Atrial fibrillation (possible flutter waves in V1), AV dissociation with complete heart block, with wide complex ventricular escape rhythm at 30 bpm
DDx for bradycardia:
- Acute ischemia
- Cardiomyopathy (ischemic or nonischemic)
- Medications (beta blockers, calcium channel blockers, digoxin, clonidine)
- Hyperkalemia
- Hypothermia
- Hypothyroidism
- Sarcoidosis/Amyloidosis
- Infectious (Lyme disease)
- Elevated Intracranial Pressure
Management of complete heart block:
- For acutely unstable patients: initiate transcutaneous pacing (patient will require sedation and pain control)
- Ventricular escape rhythms are inherently unstable, these patients must have a temporary transvenous pacemaker placed while awaiting permanent pacemaker placement
- For a comprehensive post on transvenous pacemaker placement, check out this fantasic review
Patient management and outcome:
- Pacer pads placed on patient's chest, but no pacing initiated given lack of hypotension, chest pain, altered mental status, or other indications of hypoperfusion
- STAT CT head and cspine negative for trauma
- Labs demonstrated negative hsTN and no electrolyte derangements to explain bradycardia
- While setting up for transvenous pacemaker placement, pt had a brief episode of asystole with associated loss of consciousness, this resolved after ~10 seconds of chest compressions
- Transvenous pacemaker placed, but pt's ventricular rhythm increased to 70 bpm (accelerated idioventricular rhythm) with blood pressure of 170 systolic so pacing was not initiated
- Patient admitted to CCU and received a permanent pacemaker later in the day
Take home pearls:
- Complete heart block with ventricular escape rhythms are likely to decompensate and require emergency transvenous pacemaker placement, even if seemingly stable at first
- Periodic review of the steps to perform this complicated procedure is a must for the EM physician....again check it out here!