Critical Cases - Saddle Pulmonary Embolism!
Tue, 05/04/2021 - 5:11am
Editor:
History
- 68 yo male hx of HTN, OSA, prior DVT 12 years prior not on anticoagulation presents with acute onset diffuse weakness
- States he has chest "heaviness" and dyspnea
- Notes only worsening "sciatica" pain in his R leg over the prior 3 weeks
Physical Exam
VS 97.5 HR 97 RR 22 BP 131/44 Pox 93% on 2 L by nasal canula
- General: Ill appearing. Tachypneic
- Lungs: Clear
- Heart: no murmurs
- Abd: soft and nontender
- Extrem: no noticeable edema
- Neuro: awake and alert, no focal deficits
ECG:
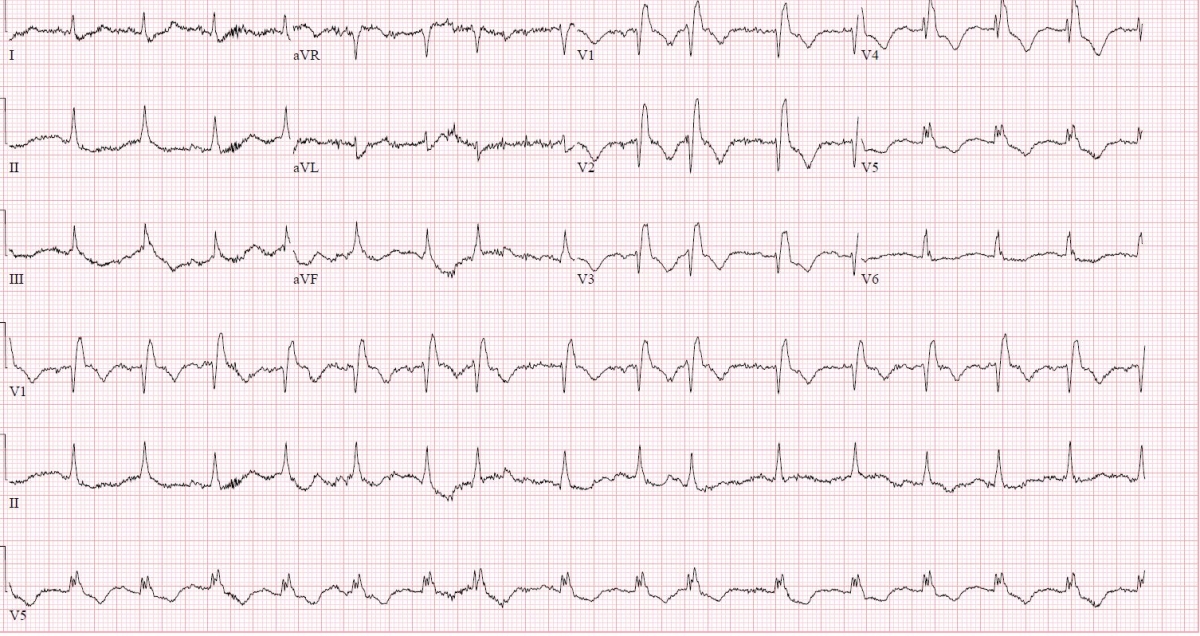
ECG interp: NSR, RBBB, TWI inferior and anterior, no ST changes
Bedside ultrasound:

4 chamber cardiac ultrasound: RV approximately the same size as LV, with hypokinesis of RV wall except for the RV apex "McConnell's sign"
Bedside 2 point compression ultraosund: +noncompressible R popliteal vein with +echogenic material
Assessment and Initial Management:
- Based on symptoms of dyspnea, tachypnea on exam, new RBBB with inferior/anterior TWI on ECG, and bedside ultrasound finding of DVT of R popliteal and dilated RV with impaired wall motion but preserved apical contractility....
- Presumptive diagnosis of pulmonary embolism was made
- Pt administed heparin bolus and infusion
- Brought emergently for CT chest
CT chest:

CT chest interpretation: saddle pulmonary embolism
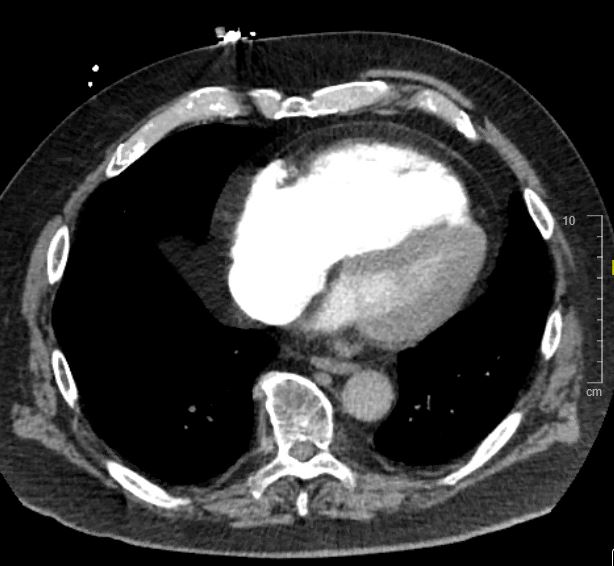
CT chest: Evidence of RV strain. Note RV is larger than LV.
Further Management
- After return from CT, pt noted to be hypotensive to 70/42 which is sustained for 10 minutes despite 1 L fluid bolus
- Decision made to administer alteplase
- 50 mg alteplase administered over 15 minutes with no change in BP
- An additional 50 mg alteplase bolus over one hour administered
- Due to ongoing hemodynamic instability, pt brought for emergency open thrombectomy


- Extensive pulmonary emboli extracted in the OR
- Pt did well and was off vasopressor support by the following day
Teaching points
- Suspect acute pulmonary embolism as a cause of undifferentiated shock
- ECG findings may include new RBBB and/or TWI in the inferior and anterior leads
- Bedside ultrasound evidence of massive PE may include RV dilation (at least as large the the LV), McConnell's sign (akinesis of the RV wall sparing the apex), or the "D" sign on parasternal short axis, or "clot in transit"
- A patient with acute onset of chest discomfort and dyspnea with a bedside ultrasound showing a DVT should be empiricially heparinized for pulmonary embolism while awaiting definitive studies
- Patients with hemodynamic instability i.e. systolic BP <90 for at least 15 minutes not due to another cause should receive systemic thrombolysis with alteplase (typically 100 mg over 2 hrs, but rapid infusion protocols exist such as 50 mg over 15 minutes)
- Half dose thrombolysis may also be considered, with similar efficacy as full dose