Deflated? Esophageal pressure monitoring in ARDS
Lung protective ventilation limiting tidal volume and plateau pressure improves survival in ARDS. The application of positive end-expiratory pressure (PEEP) further stabilizes the lung by preventing alveolar collapse during expiration, thereby reducing cyclic atelectasis. However, the optimal approach to PEEP titration to minimize ventilator-induced lung injury (VILI) has not been delineated. Numerous methods have been utilized to adjust PEEP in ARDS, including titration to optimal oxygenation or driving pressure (△P = Vt/CRS) as well as ARDSnet PEEP tables. Titrating PEEP to arterial oxygenation or empirical targets fails to account for mechanical properties of the lung or chest wall. While driving pressure measurements incorporate lung mechanics, chest wall compliance is not considered. Yet we know that reduced chest wall compliance, as seen in obesity, pregnancy or other etiologies of increased thoracoabdominal pressure, can lead to underdosing PEEP when pleural pressure is elevated.
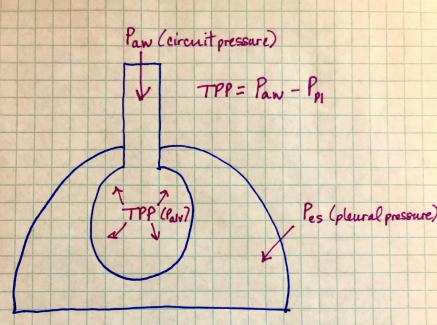
In order to avoid alveolar underdistention or overdistention, both the pressure inside the alveolus (i.e. airway circuit pressure measured by the ventilator) and outside the alveolus (pleural pressure) arguably must be known. When an esophageal pressure monitor is used to estimate esophageal pressure (Pes) as a surrogate for pleural pressure, the transpulmonary pressure (TPP), or the alveolar distending pressure, can be calculated by subtracting the pleural pressure (Ppl) from the airway circuit pressure (Paw), see figure 1. The goal of applied PEEP is to recruit nonaerated lung while avoiding overdistention of normally aerated alveoli. Esophageal manometry enables PEEP to be titrated to maintain a positive transpulmonary pressure at end-expiration, while limiting transpulmonary pressure during inspiration to a level that is lung protective.
Figure 1.
In 2008, Talmor et al. performed the EPVent-1 randomized controlled trial comparing PEEP guided by ARDSnet tables to PEEP titrated to end-expiratory transpulmonary pressure as measured by esophageal manometry. The authors hypothesized that adjusting PEEP to positive transpulmonary pressure between 0 and 10 cm H20 measured at end expiration (while limiting end-inspiratory transpulmonary pressure to < 25 cm H20 for lung protection) would improve oxygenation. Patients in both groups were ventilated with low tidal volume set at 6 mL/kg of predicted body weight and plateau pressure was maintained < 30 cm H20 targeting a PaO2 of 55 to 120 mm Hg. This pilot study was stopped early after 61 patients were enrolled, because the PaO2/FiO2 ratio in the esophageal pressure-guided group was significantly higher than the ARDSnet PEEP table group by 88 mm Hg (P = 0.0002, CI 78.1-98.3). The esophageal pressure-guided group also had improved respiratory system compliance (CRS = Vt/△P) of 45 mL/cm H20 versus 35 mL/cm H20 with P = 0.005. The mean PEEP level in the esophageal manometry group was 17 cm H20 vs 10 cm H20 in the conventional group with plateau pressure 28 cm H20 and 25 cm H20, respectively. There was no difference in transpulmonary pressure between the two groups; however, in 39 percent of the conventional group, the transpulmonary pressure at end expiration was between -1 and -6 cm H20 suggestive of alveolar collapse due to inadequate PEEP. At 28 days, mortality was lower in the esophageal pressure-guided group, although the difference was not significant (P = 0.06). Additionally, after adjustment for baseline APACHE II score, 28-day mortality in the esophageal pressure-guided group was significantly lower than the conventional group with a relative risk of 0.46 and p-value of 0.049. This mortality difference was not observed at 180 days, although separation between the Kaplan-Meier curves was maintained at this later time point. Ultimately, the authors demonstrated that esophageal pressure-guided PEEP titration was feasible, safe, and improved oxygenation without elevating transpulmonary pressure with a trend toward increased survival.
More recently in 2019, Beitler et al. performed the EPVent-2 trial comparing esophageal pressure-guided PEEP with empirical high PEEP based on the high ARDSnet PEEP-FiO2 table in a sicker population of moderate to severe ARDS patients. Esophageal pressure-guided PEEP titration in this study did not improve the composite end point incorporating mortality and ventilator-free days within 28 days. The lack of outcome difference may be accounted for by the use of empiric high PEEP in EPVent-2 versus the low ARDSnet PEEP table in EPVent-1. Accordingly, there was no significant difference in applied PEEP between the two groups (PEEP was 14 cm H20 in the esophageal pressure-guided group versus 12.5 cm H20 in the empirical high PEEP group). The authors assumed a large absolute reduction in mortality of 10 percent in their sample size calculation. Utilization of a large treatment effect size like this produces higher confidence intervals around clinical outcomes, making the trial underpowered to detect smaller, but clinically significant differences in survival. Notably, 3 times more patients in the empirical high PEEP group were treated with prone positioning and ECMO. Although this difference was not significant, it could have diluted a positive treatment effect.
Finally, Wang et al. randomized severe ARDS patients requiring VV ECMO to receive PEEP titration guided by transpulmonary pressure versus a lung rest strategy recommended by ELSO consisting of pressure assist-control ventilation with peak inspiratory pressure of 20 to 25 cm H20, PEEP 10-15 cm H30, respiratory rate 10 breaths per minute and FiO2 < 0.5. In total, 102 patients underwent randomization to a conventional lung rest strategy versus transpulmonary pressure-guided PEEP titration. The primary outcome was defined by successful weaning from ECMO with stable oxygenation and no need to reestablish ECMO. They also assessed mortality at 60 days as a secondary end point. The authors found that a greater proportion of patients were weaned from VV ECMO in the transpulmonary pressure-guided PEEP group than the conventional lung rest group (71.8% vs 48%). Lung mechanics were also better in the esophageal pressure monitoring group where lower driving pressure, tidal volume and mechanical power and higher PEEP were observed. Moreover, the transpulmonary pressure-guided group had significantly lower mortality at 60 days and 6 months as well as shorter ECMO duration and significantly less multiorgan failure. Interestingly, cytokine levels were also significantly lower in the transpulmonary pressure-guided group, which could explain lower rates of multiorgan failure. Unlike in EPVent-2, a similar proportion of patients received prone positioning in each group (78% in the esophageal pressure group vs. 76% in the lung rest group). It should be noted that this trial was limited by a relatively small sample size and single-center design.
It is difficult to reconcile the disparate results of these 3 randomized control trials examining the role of esophageal manometry for PEEP titration in ARDS. Based on the bulk of the literature, it is difficult to argue that esophageal pressure monitor-guided PEEP titration definitively improves survival in mild to moderate ARDS. However, the most recent study by Wang et al. demonstrates a profound benefit of transpulmonary pressure-guided PEEP titration in the sickest severe ARDS patients requiring VV ECMO as evidenced by greater ECMO weaning, improved short and long-term survival as well as shorter ECMO duration and less multiorgan failure. The median PaO2/FiO2 ratio of 57 mm Hg in Wang et al. as compared to 95 mm Hg in EPVent-2 and 147 mm Hg in EPVent-1 speaks to the difference in severity of lung injury in these 3 trials. Unlike in EPVent-2, the PEEP level in Wang's study was significantly higher in the transpulmonary pressure group than the conventional lung rest group. Thus, perhaps the survival benefit can be explained by simply utilizing higher empiric applied PEEP levels rather than individualized PEEP titration to transpulmonary pressure that requires invasive monitoring that is not widely available.
Based on the cumulative data, airway pressure alone may not be adequate to guide PEEP titration in subpopulations of ARDS. No single approach to PEEP titration has been prospectively proven to be superior. In my opinion, we need to pursue further study of transpulmonary pressure-guided PEEP titration in ARDS with reinflated interest to identify which subpopulations of ARDS may benefit. Similar to prone positioning, it appears that the most severe subset of ARDS patients may benefit the most from esophageal manometry, as suggested by the recent trial by Wang et al. Additionally, the role of esophageal pressure monitoring in patients with high estimated pleural or intraabdominal pressure, e.g. pregnancy, morbid obesity or pleural effusion, should be investigated to determine whether this population would benefit from PEEP guided by esophageal pressure-monitoring to ensure positive transpulmonary pressure and prevention of end-expiratory alveolar collapse.
References:
Beitler JR et al. Effect of titrating PEEP with an esophageal pressure-guided strategy vs an empirical high PEEP-FiO2 strategy on death and days free from mechanical ventilation among patients with ARDS (EPVent-2). JAMA2019;321(9):846-57.
Talmor D et al. Mechanical ventilation guided by esophageal pressure in acute lung injury (EPVent-1). New Engl J Med 2008;359(20):2095-104.
Wang R et al. Mechanical ventilation strategy guided by transpulmonary pressure in severe ARDS treated with VV ECMO. Critical Care Medicine. Advance online publication. 2020 Jun 25. doi: 10.1097/CCM.0000000000004445.