What's the Diagnosis? By Dr. Sydney Tabaac
Wed, 09/16/2020 - 11:00am
Editor:
A 17 yo F with no PMHx presents to Urgent Care w/ L sided chest pain. Pain sharp, radiates to L upper back, has been intermittent x 1 month, worse x last 2-3 days. No exacerbating or relieving factors. She denies fever/chills, cough/URI sx, LE pain/edema. No prior hx of DVT, no OCPs. On exam, she is anxious appearing. She is tachycardic to the 120s with normal heart sounds. Spo2 is 100% and breath sounds are diminished on the left. A CXR is done and shown below. What's the diagnosis?(scroll down for answer)
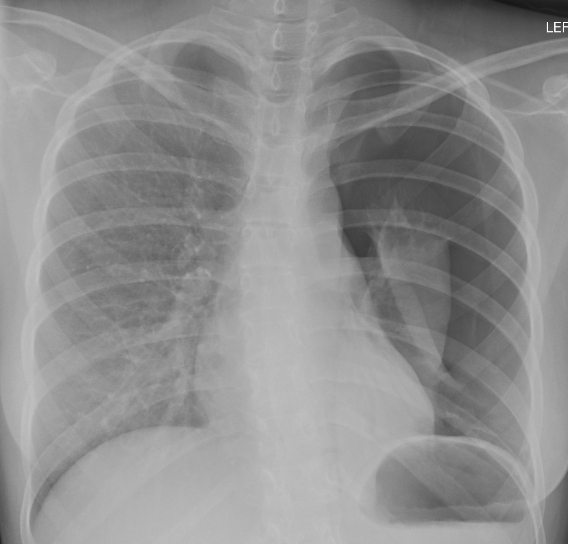
Answer: Large L sided spontaneous pneumothorax
- Types of pneumothorax:
- Primary PTX: no prior history of lung disease
- Secondary PTX: known lung disease (COPD, asthma, CF, ILD, cancer)
- Iatrogenic: secondary to invasive procedures (ie: subclavian central line)
- Tension PTX: positive pressure within pleural space
- Differential: PE, pneumonia, pericardidits, pleural effusion, shingles
- Mimics: large emphysematous bullae
- Do NOT insert chest tube
- Obtain CT or perform bedside US to differentiate
- ED treatment
- Tension PTX: CLINICAL diagnosis--> needle decompress --> tube thoracostomy
- Administer O2
- Small PTX (<20%): supplemental O2, 4 hours observation, repeat CXR
- IF improved --> follow up in 24 hours then weekly if resolves
- Aspiration or tube thoracostomy
- Needle aspiration: 14-G (adults) or 18-G (peds) at 2nd intercostal midclavicular space or 4-5th mid axillary
- Chest tube thoracostomy: 10 to 14 Fr if nontraumatic; 14 to 22 Fr if large air leak suspected
- Further management in this case:
- Transferred to hospital
- Placement of 16 Fr thorcostomy by peds surgery at bedside
- Chest tube placed to suction x 48 h then waterseal
- repeat CXR at 4 hours of waterseal revealed no PTX
- Chest tube pulled and follow up CXR at 5 hours post removal was stable--> patient discharged
References: